Chapter 11 Rheumatology and bone disease
Rheumatological and musculoskeletal disorders
Many common locomotor problems are short-lived and self-limiting or settle with a course of simple analgesia and/or physical treatment; e.g. physiotherapy or osteopathy. However, they represent 20–30% of the workload of the primary care physician, where non-inflammatory problems predominate. Recognition and appropriate early treatment of many painful rheumatic conditions may help reduce the incidence of chronic pain disorders. Early recognition and subsequent treatment of inflammatory arthritis by specialist multidisciplinary teams leads to better symptom control and prevents long-term joint damage and disability. The patient should always be included when decisions about treatment are being discussed. Pamphlets and websites offer helpful advice for patients, and their use should be encouraged.
The normal joint
There are three types of joints: fibrous, fibrocartilaginous and synovial.
Fibrous and fibrocartilaginous joints
These include the intervertebral discs, the sacroiliac joints, the pubic symphysis and the costochondral joints. Skull sutures are fibrous joints.
Synovial joints
These (Fig. 11.1) include the ball-and-socket joints (e.g. hip) and the hinge joints (e.g. interphalangeal).
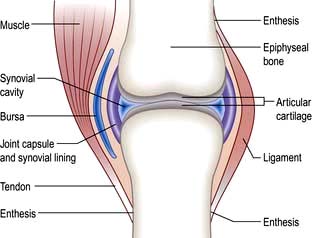
They possess a cavity and permit the opposed cartilaginous articular surfaces to move painlessly over each other. Movement is restricted to a required range, and stability is maintained during use. The load is distributed across the surface, thus preventing damage by overloading or disuse.
Synovium and synovial fluid. The joint capsule, which is connected to the periosteum, is lined with synovium, which is a few cells thick and vascular. Its surface is smooth and non-adherent and is permeable to proteins and crystalloids. As there are no macroscopic gaps, it is able to retain normal joint fluid even under pressure. Macrophages and fibroblast-like synoviocytes form the synovial layer by cell-to-cell interactions mediated by cadherin-II. The synoviocytes release hyaluronan into the joint space, which helps to retain fluid in the joint. Synovial fluid is a highly viscous fluid secreted by the synovial cells and has a similar consistency to plasma. Glycoproteins ensure a low coefficient of friction between the cartilaginous surfaces. Tendon sheaths and bursae are also lined by synovium.
Juxta-articular bone
The bone which abuts a joint (epiphyseal bone) differs structurally from the shaft (metaphysis) (see Fig. 11.32). It is highly vascular and comprises a light framework of mineralized collagen enclosed in a thin coating of tougher, cortical bone. The ability of this structure to withstand pressure is low and it collapses and fractures when the normal intra-articular covering of hyaline cartilage is worn away as in osteoarthritis (OA; see p. 512). Loss of surface cartilage also leads to the abnormalities of bone growth and remodelling typical of OA (see p. 512).
Hyaline cartilage
Hyaline cartilage forms the articular surface and is avascular. It relies on diffusion from synovial fluid for its nutrition. It is rich in type II collagen that forms a meshwork enclosing giant macromolecular aggregates of proteoglycan. These heterogeneous macromolecules comprise protein chains with side-chains of the carbohydrates keratan and chondroitin sulphate (aggrecans). These molecules have a negative charge and retain water in the structure by producing a dynamic tension between the retaining force of the collagen matrix and the expansive effect of osmotic pressure. Intermittent pressure from ‘loading’ of the joint is essential to normal cartilage function and encourages movement of water, minerals and nutrients between cartilage and synovial fluid. Chondrocytes secrete collagen and proteoglycans and are embedded in the cartilage. They migrate towards the joint surface along with the matrix they produce.
Ligaments and tendons
These structures stabilize joints. Ligaments are variably elastic and this contributes to the stiffness or laxity of joints (see p. 559). Tendons are inelastic and transmit muscle power to bones. The joint capsule is formed by intermeshing tendons and ligaments. The point where a tendon or ligament joins a bone is called an enthesis and may be the site of inflammation.
Components of extracellular matrix
All connective tissues contain an extracellular matrix of macromolecules: collagens, elastins, non-collagenous glycoproteins and proteoglycans, in addition to cells, e.g. synoviocytes. There are several different types of cell surface receptors that bind extracellular matrix proteins including the integrins, CD44 and the proteoglycan family of receptors, e.g. syndecans.
Collagens. Collagens consist of three polypeptide (α) chains wound into a triple helix. These alpha chains contain repeating sequences of Gly-x-y triplets, where x and y are often prolyl and hydroxypropyl residues. Collagen fibres show genetic heterogeneity, with genes on at least 12 chromosomes. Hyaline cartilage is 90% type II (COL2A1). There are several classes of collagen genes, based on their protein structures, and abnormalities of these may lead to specific diseases (see p. 560).
Elastin, secreted as tropoelastin, is an insoluble protein polymer and is the main component of elastic fibres.
Glycoproteins. Fibronectin is the major non-collagenous glycoprotein in the extracellular matrix. Its molecule contains a number of functional domains, or cell recognition sites that bind ligands and are involved in cellular adhesion. Fibronectin plays a major role in tissue remodelling. Its production is stimulated by interferon-gamma (IFN-γ) and by transforming growth factor-beta and inhibited by tumour necrosis factor and interleukin-1.
Proteoglycans. These proteins contain glycosaminoglycan (GAG) side-chains and are of variable form and size. Many different molecules have been identified at different sites in connective tissue. Their function is to bind extracellular matrix together, retain soluble molecules in the matrix and assist with cell binding. Abnormalities of any of these structures may lead to periarticular or articular symptoms and/or predispose to the development of arthritis.
Joint sensation
The ligaments, periosteum, synovial tissue and capsule of the joint are richly supplied by blood vessels and nerves. Pain usually derives from inflammation of these sites because the synovial membrane is relatively insensitive.
Connective tissue degradation
Connective tissue constantly undergoes repair and re-modelling. Degradation is mediated by enzymes such as aggrecanase and matrix metalloproteinases (MMPs) which require zinc and act at a neutral pH. There are several MMPs which act on different collagens, e.g. the gelatinases (MMP-2 and -9), which degrade denatured collagen. MMPs also act on non-collagen proteins, e.g. the stromelysins (MMP-3, -10, -11), which degrade proteoglycans and fibronectin.
The turnover of normal collagen is initiated by cytokines, e.g. interleukin-1 synthesized by chondrocytes. Activation of latent MMPs and tissue plasminogen activator then occurs.
Two inhibitors, TIMP (Tissue Inhibitor of Metalloproteinase) and plasminogen activator inhibitor-1 (PAI-1), inhibit degradation during matrix remodelling.
Skeletal muscle
This consists of bundles of myocytes containing actin and myosin molecules. These molecules interdigitate and form myofibrils which cause muscle contraction in a similar way to myocardial muscle (p. 671). Bundles of myofibrils (fasciculi) are covered by connective tissue, the perimysium, which merges with the epimysium (covering the muscle) and forms the tendon which attaches to the bone surface (enthesis).
Clinical approach to the patient
Taking a musculoskeletal history
The following questions are helpful in assessing the problem and making a diagnosis. A history can often lead to a diagnosis as pattern recognition is the key to diagnosis in rheumatic diseases.
 Where is it? Is it localized or generalized? The pattern of joint involvement is a useful clue to the diagnosis (e.g. distal interphalangeal joints in nodal osteoarthritis).
Where is it? Is it localized or generalized? The pattern of joint involvement is a useful clue to the diagnosis (e.g. distal interphalangeal joints in nodal osteoarthritis).
Is it arising from joints, the spine, muscles or bone, with local tenderness? Soft tissue lesions and inflamed joints are locally tender.
Could it be referred from another site? Joint pain is localized but may radiate distally – shoulder to upper arm; hip to thigh and knee.
Is it constant, intermittent or episodic? How severe is it – aching or agonizing?
Are there aggravating or precipitating factors? Is it made worse by activity and eased by rest (mechanical) or worse after rest (inflammatory).
Are there any associated neurological features? Numbness, pins and needles and/or loss of power suggest ‘nerve’ involvement. The distribution of symptoms is a useful clue to the nerve or nerve root affected.
Is it generalized or localized? Spine or joint stiffness is common after injury.
Does it affect the limb girdles or periphery?
Is it worse in the morning and relieved by activity?
Gout (see p. 530), reactive arthritis (p. 529) and ankylosing spondylitis (p. 527) are more common in men. Rheumatoid arthritis and other autoimmune rheumatic diseases are more common in women.
Is there any associated ill-health or other worrying feature, such as weight loss or fever?
Are there other associated medical conditions that may be relevant? Psoriasis (see p. 1207) or inflammatory bowel disease is associated with spondyloarthritis (see p. 1004). Charcot’s joints (p. 547) are seen in diabetics.
Could a drug be a cause? Diuretics may precipitate gout in men and older women. Hormone replacement therapy or the oral contraceptive pill may precipitate systemic lupus erythematosus (SLE) (p. 535). Steroids can cause avascular necrosis. Some drugs cause a lupus-like syndrome (p. 535).
Is this relevant? Sickle cell disease causes joint pain in young black Africans, but osteoporosis (see p. 552) is uncommon in older black Africans.
Have there been any similar episodes or is this the first? Are there any clues from previous medical conditions? Gout is recurrent; the episodes settle without treatment in 7–10 days. Acute episodes of palindromic rheumatism may predate the onset of rheumatoid arthritis (see p. 519).
What job does the patient do? This can be a factor in soft tissue problems and osteoarthritis (e.g. in heavy labourers and dancers). Work-related problems, particularly in those who use a keyboard, are becoming more common and are complained of more.
The biopsychosocial model of disease is highly relevant to many rheumatic disorders:
Has there been any recent major stress in family or working life? Could this be relevant? Stress rarely causes rheumatic disease but may precipitate a flare-up of inflammatory arthritis. It reduces a person’s ability to cope with pain or disability.
Has there been an injury for which a legal case for compensation is pending?
The World Health Organization describes the impact of disease on an individual in terms of:
Impairment: any loss or abnormality of psychological or anatomical structure or function
Disability (activity limitation): any restriction or lack of ability to perform an activity in the manner or within the range considered normal for a human being
Handicap (participation restriction): a disadvantage for an individual resulting from an impairment or disability that limits or prevents the fulfilment of a role that is normal for that individual.
The patient’s own perception of limitation must be taken into account during assessment, as well as the impact of physical causes due to disease. Subjective and objective assessments must be made. Quality of life (QoL) involves physical and psychosocial factors. The aim of treatment is to reduce or cure physical and/or psychological disease and to reduce the impact of any impairment or disability on the individual. A variety of different standard questionnaires is used to assess pain, disease impact and outcome (e.g. Health Assessment Questionnaire, HAQ; Arthritis Impact Measurement Scale, AIMS).
Examination of the joints
Always observe a patient, looking for disabilities, as he or she walks into the room and sits down. General and neurological examinations are often necessary. Guidelines for rapid examinations of the limbs and spine are shown in Practical Box 11.1.
 Practical Box 11.1
Practical Box 11.1
Rapid examinations of the limb and spine
Rapid examination of the upper limbs
Raise arms sideways to the ears (abduction). Reach behind neck and back. Difficulties with these movements indicate a shoulder or rotator cuff problem.
Hold the arms forward, with elbows straight and fingers apart, palm up and palm down. Fixed flexion at the elbow indicates an elbow problem. Examine the hands for swelling, wasting and deformity.
Place the hands in the ‘prayer’ position with the elbows apart. Flexion deformities of the fingers may be due to arthritis, flexor tenosynovitis or skin disease. Painful restriction of the wrist limits the person’s ability to move the elbows out with the hands held together.
Make a tight fist. Difficulty with this indicates a loss of flexion or grip. Grip strength can be measured.
Rapid examination of the lower limbs
Ask the patient to walk a short distance away from and towards you, and to stand still. Look for abnormal posture or stance.
Ask the patient to stand on each leg. Severe hip disease causes the pelvis on the non-weight-bearing side to sag (positive Trendelenburg test).
Watch the patient stand and sit, looking for hip and/or knee problems.
Ask the patient to straighten and flex each knee.
Ask the patient to place each foot in turn on the opposite knee with the hip externally rotated. This tests for painful restriction of hip or knee. Abnormal hips or knees must be examined lying.
Move each ankle up and down. Examine the ankle joint and tendons, medial arch and toes whilst standing.
Rapid examination of the spine
Ask the patient to (a) bend forwards to touch the toes with straight knees, (b) extend backwards, (c) flex sideways, and (d) look over each shoulder, flexing and extending and sideflexing the neck. Observe abnormal spinal curves – scoliosis (lateral curve), kyphosis (forward bending) or lordosis (backward bending). A cervical and lumbar lordosis and a thoracic kyphosis are normal. Muscle spasm is worse whilst standing and bending. Leg length inequality leads to a scoliosis which decreases on sitting or lying (the lengths are measured lying).
Ask the patient to lie supine. Examine any restriction of straight-leg raising (see disc prolapse, below).
Ask the patient to lie prone. Examine for anterior thigh pain during a femoral stretch test (flexing knee whilst prone), which indicates a high lumbar disc problem.
Examining an individual joint involves three stages: looking, feeling and moving (Table 11.1). A screening examination of the locomotor system, known by the acronym GALS (Global Assessment of the Locomotor System) has been devised. X-ray or ultrasound of the joint often forms an integral part of the examination.
Table 11.1 Examination of the joint
LOOK at the appearance of the joint |
Swelling – could be bony, fluid or synovial |
Deformity – valgus, where the distal bone is deviated laterally (e.g. knock-knees or genu valgum) |
|
Varus where the distal bone is deviated medially (bow-legs or genu varum) |
|
Fixed flexion or hyperextension |
|
Rash – especially psoriasis |
|
Muscle wasting – easier to see in large muscles like the quadriceps |
|
Scars – from surgery or trauma |
|
Signs of inflammationSymmetry – are the right and left joints (e.g. hips, knees, any other paired joint) the same? If not which do you think is abnormal? |
|
FEEL |
Swelling – fluid swelling (effusion) usually represents increased synovial fluid in inflammatory arthritis, but can be due to blood or pus |
Synovial swelling is rubbery or boggy and usually occurs in inflammatory arthritis |
|
Bony swelling, such as Heberden’s nodes in the fingers is usually seen in osteoarthritis |
|
Warmth – a warm joint may be inflamed or infected |
|
Tenderness – may represent joint inflammation, but many people have chronic tenderness all over the body (e.g. in fibromyalgia) |
|
MOVE |
Active movement – is the range full and pain-free? Is the movement fluid? In the hands – can the patient perform fine movements? In the legs – can the patient walk properly? |
Compare movements on the right and left side – are they symmetrical? |
|
Is there crepitus when the joint is moved? |
|
If active movement is limited try passive movement. In a joint problem both will usually be affected. If it is a muscle or nerve problem passive movement may remain full. |
Investigations
Investigations are unnecessary in many of the common musculoskeletal problems; the diagnosis is clear from the history and examination findings. Tests help to exclude another condition and to reassure the patient or their primary care physician.
Useful blood screening tests
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). An increase of these reflects inflammation. Plasma viscosity is also raised in inflammatory disease.
Bone and liver biochemistry. A raised serum alkaline phosphatase may indicate liver or bone disease. A rise in liver enzymes is seen with drug-induced toxicity. For other investigations of bone, see page 550.
Serum autoantibody studies
Rheumatoid factors (RFs) (see also p. 518). Rheumatoid factors are detected by enzyme linked immunoabsorbent assay (ELISA). RFs are antibodies (usually IgM, but also IgG or IgA) against the Fc portion of IgG. They are detected in 70% of people with rheumatoid arthritis (RA), but are not diagnostic. RFs are detected in many autoimmune rheumatic disorders (e.g. SLE), in chronic infections, and in asymptomatic older people (Table 11.2).
Anti-citrullinated peptide antibodies (ACPA). These antibodies are directed against citrullinated antigens, vimentin, fibrinogen, alpha enolase and type II collagen. They are measured by an ELISA technique and are present in up to 80% of people with RA. They have a high specificity for RA (90% with a sensitivity of 60%). They are helpful in early disease when the RF is negative to distinguish it from acute transient synovitis (see Box 11.6, p. 519). Positivity for RF and/or ACPA is associated with a worse prognosis and an increase in the likelihood of bony erosions in people with RA.
Antinuclear antibodies (ANAs). These are detected by indirect immunofluorescent staining of fresh-frozen sections of rat liver or kidney or Hep-2 cell lines. Different patterns reflect a variety of antigenic specificities that occur with different clinical pictures (see Box 11.16, p. 537). ANA is used as a screening test for systemic lupus erythematosus (SLE) and systemic sclerosis (SSc) – a negative ANA makes either condition highly unlikely – but low titres occur in RA and chronic infections and in normal individuals, especially the elderly (Table 11.3).
Anti-double-stranded DNA (dsDNA) antibodies. These are usually detected by a precipitation test (Farr assay), by ELISA, or by an immunofluorescent test using Crithidia luciliae (which contains double-stranded DNA). Raised anti-dsDNA is highly specific for SLE and the levels usually rise and fall in parallel with disease activity so can be used to monitor the level of treatment required.
Anti-extractable nuclear antigen (ENA) antibodies (see Box 11.16, p. 537). These produce a speckled ANA fluorescent pattern, and can be identified by ELISA. The most commonly measured ENAs are:
Anti-neutrophil cytoplasmic antibodies (ANCAs) (see p. 544). These are predominantly IgG autoantibodies directed against the primary granules of neutrophil and macrophage lysosomes. They are strongly associated with small-vessel vasculitis. Two major clinically relevant ANCA patterns are recognized on immunofluorescence:
Antiphospholipid antibodies (see p. 538). These are detected in the antiphospholipid syndrome (see p. 538).
Immune complexes. Immune complexes are infrequently measured, largely because of variability between assays and difficulty in interpreting their meaning. Assays based on the polyethylene glycol precipitation method (PEG) or C1q binding are available commercially.
Complement. Low complement levels indicate consumption and suggest an active disease process in SLE.
Table 11.2 Conditions in which rheumatoid factor is found in the serum
Autoimmune rheumatic diseases |
RF (IgM) % |
Rheumatoid arthritis |
70 |
Systemic lupus erythematosus |
25 |
Sjögren’s syndrome |
90 |
Systemic sclerosis |
30 |
Polymyositis/dermatomyositis |
50 |
Juvenile idiopathic arthritis |
Variable |
Viral infections |
Hyperglobulinaemias |
Hepatitis |
Chronic liver disease |
Infectious mononucleosis |
Sarcoidosis |
Cryoglobulinaemia |
|
Chronic infections |
Normal population |
Tuberculosis |
Elderly |
Leprosy |
Relatives of people with RA |
Syphilis |
|
Table 11.3 Conditions in which serum antinuclear antibodies are found
| (%) | |
|---|---|
Systemic lupus erythematosus |
95 |
Systemic sclerosis |
70 |
Sjögren’s syndrome |
80 |
Polymyositis and dermatomyositis |
40 |
Rheumatoid arthritis |
30 |
Juvenile idiopathic arthritis |
Variable |
Other diseases |
|
Autoimmune hepatitis |
100 |
Drug-induced lupus |
>95 |
Myasthenia gravis |
50 |
Idiopathic pulmonary fibrosis |
30 |
Diabetes mellitus |
25 |
Infectious mononucleosis |
5–10 |
Normal population |
8 |
Joint aspiration
Examination of joint (or bursa) fluid is used mainly to diagnose septic, reactive or crystal arthritis. The appearance of the fluid is an indicator of the level of inflammation. The procedure is often undertaken in combination with injection of a corticosteroid. Aspiration alone is therapeutic in crystal arthritis (see Practical Box 11.2, p. 508).
Examination of synovial fluid
Aspiration and analysis of synovial fluid are always indicated when an infected or crystal induced arthritis is suspected, particularly a monoarthritis. Normal fluid is clear and straw coloured and contains <3000 WBC/mm3. Inflammatory fluid is cloudy and contains >3000 WBC/mm3. Septic fluid is opaque and less viscous and contains up to 75 000 WCC/mm3. There is much overlap.
Polarized light microscopy is performed for crystals.
Gout: negatively birefringent, needle-shaped crystals of sodium urate
Pyrophosphate arthropathy (pseudogout): rhomboidal, weakly positively birefringent crystals of calcium pyrophosphate.
Gram staining is essential if septic arthritis is suspected and may identify the organism immediately. Joint fluid should be cultured and antibiotic sensitivities requested.
Diagnostic imaging and visualization
X-rays can be diagnostic in certain conditions (e.g. established rheumatoid arthritis) and are the first investigation in many cases of trauma. X-rays can detect joint space narrowing, erosions in rheumatoid arthritis, calcification in soft tissue, new bone formation, e.g. osteophytes and decreased bone density (osteopenia) or increased bone density (osteosclerosis):
Ultrasound (US) is particularly useful for periarticular structures, soft tissue swellings and tendons and for detecting active synovitis in inflammatory arthritis. It is increasingly used to examine the shoulder and other structures during movement, e.g. shoulder impingement syndrome (see p. 500). Doppler US measures blood flow and hence inflammation. US is used to guide local injections.
Magnetic resonance imaging (MRI) shows bone changes and intra-articular structures in striking detail. Visualization of particular structures can be enhanced with different resonance sequences. T1-weighted is used for anatomical detail, T2-weighted for fluid detection and short tau inversion recovery (STIR) for the presence of bone marrow oedema. It is more sensitive than X-rays in the early detection of articular and periarticular disease. It is the investigation of choice for most spinal disorders but is inappropriate in uncomplicated mechanical low back pain. Gadolinium injection enhances inflamed tissue. MRI can also detect muscle changes, e.g. myositis.
Computerized axial tomography (CT) is useful for detecting changes in calcified structures but dose of irradiation is high.
Bone scintigraphy utilizes radionuclides, usually 99mTc, and detects abnormal bone turnover and blood circulation and, although nonspecific, helps in detecting areas of inflammation, infection or malignancy. It is best used in combination with other anatomical imaging techniques.
DXA scanning uses very low doses of X-irradiation to measure bone density and is used in the screening and monitoring of osteoporosis.
Positron emission tomography (PET) scanning uses radionuclides, which decay by emission of positrons. 18F-Fluorodeoxyglucose uptake indicates areas of increased glucose metabolism. It is used to locate tumours and demonstrate large vessel vasculitis, e.g. Takayasu’s arteritis (see p. 789). PET scans are combined with CT to improve anatomical details.
Arthroscopy is a direct means of visualizing a joint, particularly the knee or shoulder. Biopsies can be taken, surgery performed in certain conditions (e.g. repair or trimming of meniscal tears), and loose bodies removed.
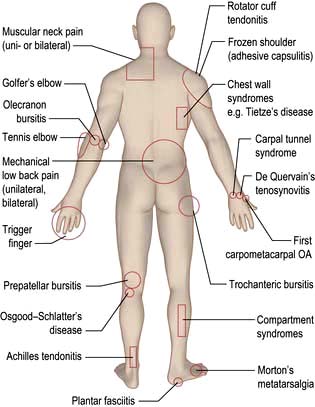
Common regional musculoskeletal problems (fig. 11.2)
Pain in the neck and shoulder (Table 11.4)
Mechanical or muscular neck pain (shoulder girdle pain)
Unilateral or bilateral muscular-pattern neck pain is common and usually self-limiting. It can follow injury, falling asleep in an awkward position, or prolonged keyboard working. Chronic burning neck pain occurs because of muscle tension from anxiety and stress.
Table 11.4 Pain in the neck and shoulder
|
Mechanical or muscular neck pain Disc prolapse – nerve root entrapment (p. 499) Fibromyalgia (chronic widespread pain) |
Spondylosis seen on X-ray increases after the age of 40 years, but it is not always causal. Spondylosis can, however, cause stiffness and increases the risk of mechanical or muscular neck pain. Muscle spasm is palpable and tender and may lead to abnormal neck posture (e.g. acute torticollis). Muscular-pattern neck pain is not localized but affects the trapezius muscle, the C7 spinous process and the paracervical musculature (shoulder girdle pain). Pain often radiates upwards to the occiput and is commonly associated with tension headaches. These features are also seen in chronic widespread pain (see p. 509).
Treatment
Patients are given short courses of analgesic therapy along with reassurance and explanation. Physiotherapists can help to relieve spasm and pain, teach exercises and relaxation techniques, and improve posture. An occupational therapist can advise about the ergonomics of the workplace if the problem is work-related (see p. 510).
Nerve root entrapment
This is caused by an acute cervical disc prolapse or pressure on the root from spondylotic osteophytes narrowing the root canal.
Acute cervical disc prolapse presents with unilateral pain in the neck, radiating to the interscapular and shoulder regions. This diffuse, aching dural pain is followed by sharp, electric shock-like pain down the arm, in a nerve root distribution, often with pins and needles, numbness, weakness and loss of reflexes (Table 11.5).
Cervical spondylosis occurs in the older patient with posterolateral osteophytes compressing the nerve root and causing root pain (see Fig. 22.58, p. 1148), commonly at C5/C6 or C6/C7; it is seen on oblique radiographs of the neck. An MRI scan clearly distinguishes facet joint OA, root canal narrowing and disc prolapse.
Treatment
A support collar, rest, analgesia and sedation are used initially as necessary. Patients should be advised not to carry heavy items. It usually recovers in 6–12 weeks. MRI is the investigation of choice if surgery is being considered or the diagnosis is uncertain (Fig. 11.3). A cervical root block administered under direct vision by an experienced pain specialist may relieve pain while the disc recovers. Neurosurgical referral is essential if the pain persists or if the neurological signs of weakness or numbness are severe or bilateral. Bilateral root pain with or without long track symptoms or signs is a neurosurgical emergency because a central disc prolapse may compress the cervical spinal cord. Posterior osteophytes may cause spinal claudication and cervical myelopathy.

Whiplash injury
Whiplash injury results from acceleration–deceleration forces applied to the neck, usually in a road traffic accident when the car of a person wearing a seat belt is struck from behind. A simple decision plan based on clinical criteria helps to distinguish those most at risk and who warrant radiography. There is a low probability of serious bony injury if there is:
CT scans are reserved for those with bony injury. MRI scans occasionally show severe soft tissue injury. Whiplash injuries commonly lead to litigation.
Whiplash injury is a common cause of chronic neck pain, although most people recover within a few weeks or months. Delayed recovery depends in part upon the severity of the initial injury. The pattern of chronic neck pain is often complex, involving pain in the neck, shoulder and arm. Subjective symptoms such as headache, dizziness, and poor concentration sometimes accompany this. The subjective nature of these symptoms has led to controversy about their cause. The problem is more commonly seen in industrialized countries where the conflictive nature of the compensation process may actually delay recovery. Non-conflictive means of compensation may lead to a better prognosis.
Treatment is with reassurance (the patient is often distressed and anxious), analgesia, a short-term support collar and physiotherapy. Pain may take a few weeks or months to settle and the patient should be warned of this.
Pain in the shoulder
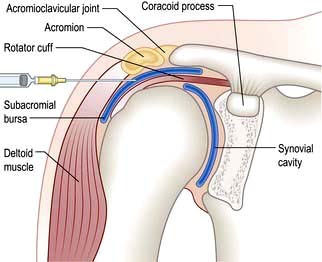
The shoulder is a shallow joint with a large range of movement. The humeral head is held in place by the rotator cuff (Fig. 11.4) which is part of the joint capsule. It comprises the tendons of infraspinatus and teres minor posteriorly, supraspinatus superiorly and teres major and subscapularis anteriorly. The rotator cuff (particularly supraspinatus) prevents the humeral head blocking against the acromion during abduction; the deltoid pulls up and the supraspinatus pulls in to produce a turning movement and the greater tuberosity glides under the acromion without impingement. Shoulder pathology restricts or is made worse by shoulder movement. Specific diagnoses are difficult to make clinically but this may not matter for pain management.
Pain in the shoulder can sometimes be due to problems in the neck. The differential diagnosis of this is shown in Box 11.1. Adhesive capsulitis (true frozen shoulder) is uncommon (see below). Early inflammatory arthritis and polymyalgia rheumatica in the elderly may present with shoulder pain. Shoulder pain is more common in diabetic patients than in the general population.
 Box 11.1
Box 11.1
Differential diagnosis of ‘shoulder’ pain
Rotator cuff tendonitis pain is worse at night and radiates to the upper arm.
Painful shoulders produce secondary muscular neck pain.
Muscular neck pain (also known as shoulder girdle pain) does not radiate to the upper arm.
Cervical nerve root pain is usually associated with pins and needles or neurological signs in the arm.
Rotator cuff (supraspinatus) tendonosis
This is a common cause of shoulder pain at all ages. It follows trauma in 30% of cases and is bilateral in under 5%. The pain radiates to the upper arm and is made worse by arm abduction and elevation, which are often limited. The pain is often worse during the middle of the range of abduction, reducing as the arm is raised fully; a so-called ‘painful arc syndrome’. When examined from behind, the scapula rotates earlier than usual during elevation. Passive elevation reduces impingement and is less painful. Severe pain virtually immobilizes the joint, although some rotation is retained (cf. adhesive capsulitis, see below). There is also painful spasm of the trapezius. There may be an associated subacromial bursitis. Isolated subacromial bursitis occurs after direct trauma, falling on to the outstretched arm or elbow. Acromioclavicular osteophytes increase the risk of impingement and may need to be removed surgically.
X-rays or ultrasound are necessary only when rotator cuff tendonosis is persistent or the diagnosis is uncertain.
Treatment
Analgesics, NSAIDs and/or physiotherapy may suffice, but severe pain responds to an injection of corticosteroid into the subacromial bursa (Fig. 11.4). Patients should be warned that 10% will develop worse pain for 24–48 hours after injection. Some 70% improve over 5–20 days and mobilize the joint themselves. Physiotherapy helps persistent stiffness. Further ultrasound-guided corticosteroid injections may be needed but the long-term benefit is unclear.
Torn rotator cuff
This is caused by trauma but also occurs spontaneously in the elderly and in rheumatoid arthritis (RA). It prevents active abduction of the arm, but patients learn to initiate elevation using the unaffected arm. Once elevated, the arm can be held in place by the deltoid muscle. In younger people, the tear is repaired surgically but this is rarely possible in the elderly or in RA. Some patients require arthroscopic surgery.
Calcific tendonosis and bursitis
Calcium pyrophosphate deposits in the tendon are visible on X-ray, but they are not always symptomatic. The pathogenesis is unclear, although ischaemia may play a part. The deposit is usually just proximal to the greater tuberosity. It may lead to acute or chronic recurrent shoulder pain and restriction of movement. A local corticosteroid injection may relieve the pain. The calcification may persist or resolve. Aspiration or breaking up of the deposit under ultrasound control may be required for persistent pain. Rarely, arthroscopic removal is necessary.
Shedding of crystals into the subacromial bursa causes a bursitis with severe pain and shoulder restriction. The shoulder feels hot and is swollen, and an X-ray shows a diffuse opacity in the bursa. The differential diagnosis of calcific bursitis is gout, pseudogout or septic arthritis. Aspiration and injection with corticosteroid can help.
Adhesive capsulitis (true ‘frozen’ shoulder)
This is uncommon but can develop with rotator cuff lesions, or following hemiplegia, chest or breast surgery or myocardial infarction. It causes severe shoulder pain and complete loss of all shoulder movements, including rotation. High doses of NSAIDs and intra-articular injections of local anaesthetic and corticosteroids are helpful. Once the pain settles, arthroscopic release speeds functional recovery.
Pain in the elbow
Pain in the elbow can be due to epicondylitis, inflammatory arthritis or occasionally osteoarthritis.
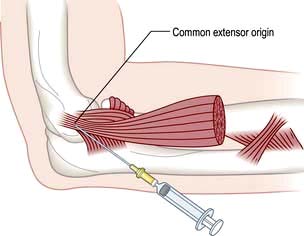
Epicondylitis
Two common sites where the insertions of tendons into bone become inflamed (enthesitis) are the insertions of the wrist extensor tendon into the lateral epicondyle (‘tennis elbow’) and the wrist flexor tendon into the medial epicondyle (‘golfer’s elbow’). Both are usually unrelated to either sporting activity.
There is local tenderness. Pain radiates into the forearm on using the affected muscles – typically, gripping or holding a heavy bag in tennis elbow or carrying a tray in golfer’s elbow. Pain at rest also occurs.
Treatment
Advise rest and arrange review by a physiotherapist. A local injection of corticosteroid at the point of maximum tenderness is helpful when the pain is severe but needs physiotherapy follow-up to prevent recurrences (Fig. 11.5). Avoid the ulnar nerve when injecting golfer’s elbow. Both conditions settle spontaneously eventually, but occasionally persist and require surgical release.
Pain in the hand and wrist (table 11.6)
Hand pain is commonly caused by injury or repetitive work-related activities. When associated with pins and needles or numbness it suggests a neurological cause arising at the wrist, elbow or neck. Pain and stiffness that are worse in the morning are due to tenosynovitis or inflammatory arthritis. The distribution of hand pain often indicates the diagnosis.
Table 11.6 Pain in the hand and wrist: causes
| All ages | Older patients |
|---|---|
Trauma/fractures |
Nodal OA: |
Tenosynovitis: |
DIPs (Heberden’s nodes) |
Flexor with/without triggering |
PIPs (Bouchard’s nodes) |
Dorsal |
|
De Quervain’s |
Trauma – scaphoid fracture |
Pseudogout |
|
Gout: |
|
Acute |
|
Tophaceous |
|
|
DIPs, PIPs, distal and proximal interphalangeal joints.
Tenosynovitis
The finger flexor tendons run through synovial sheaths and under loops which hold them in place. Inflammation occurs with repeated or unaccustomed use, or in inflammatory arthritis. The thickened sheaths are often palpable.
Flexor tenosynovitis causes finger pain when gripping and stiffness of the fingers in the morning. Occasionally a tendon causes a trigger finger, when the finger remains flexed in the morning or after gripping and has to be pulled straight. A tender tendon nodule is palpable, usually in the distal palm. Trigger finger or thumb is commoner in diabetic patients.
Dorsal tenosynovitis is less common except in rheumatoid arthritis. The hourglass swelling extends from the back of the hand and under the extensor retinaculum.
De Quervain’s tenosynovitis causes pain and swelling around the radial styloid where the abductor pollicis longus tendon is held in place by a retaining band. There is local tenderness, and the pain at the styloid is worsened by flexing the thumb into the palm.
Carpal tunnel syndrome
This is due to median nerve compression in the limited space of the carpal tunnel. Thickened ligaments, tendon sheaths or bone enlargement can cause it, but it is usually idiopathic. (Causes are discussed on p. 1144.) The history is usually typical and diagnostic with the patient waking with numbness, tingling and pain in a median nerve distribution. The pain radiates to the forearm. The fingers feel swollen but usually are not. Wasting of the abductor pollicis brevis develops with sensory loss in the radial three and a half fingers. The pain may be produced by tapping the nerve in the carpal tunnel (Tinel’s sign) or by holding the wrist in flexion (Phalen’s test).
Treatment is with a splint to hold the wrist in dorsiflexion overnight. This relieves the symptoms and is diagnostic; used nightly for several weeks it may produce full recovery. If it does not, a corticosteroid injection into the carpal tunnel (avoid the nerve!) helps in about 70% of cases, although it may recur. Persistent symptoms or nerve damage produce prolonged latency across the carpal tunnel on nerve conduction studies and require surgical decompression.
Other conditions causing pain
Inflammatory arthritis. This may present with pain, swelling and stiffness of the hands. In RA the wrists, proximal interphalangeal (PIP) joints and metacarpophalangeal (MCP) joints are affected symmetrically. In psoriatic arthritis and reactive arthritis a finger may be swollen (dactylitis) or the distal interphalangeal (DIP) joints and nails are affected asymmetrically.
Nodal osteoarthritis. This affects the DIP and less commonly PIP joints, which are initially swollen and red. The inflammation and pain settle but bony swellings remain (p. 514).
First carpometacarpal osteoarthritis. This causes pain at the base of the thumb when gripping, or painless stiffness at the base of the thumb, often in persons with nodal osteoarthritis.
Scaphoid fractures. These cause pain in the anatomical snuffbox. They are not seen immediately on X-ray. A cast is necessary. Untreated scaphoid fractures can eventually cause pain because of failed union.
Ganglion. A ganglion is a jelly-filled, often painless swelling caused by a partial tear of the joint capsule or tendon sheath. The wrist is a common site. Treatment is not essential as many resolve or cause little trouble, otherwise surgical excision is the best option.
Dupuytren’s contracture
This is a painless, palpable fibrosis of the palmar aponeurosis, with fibroblasts invading the dermis due to abnormal signalling in the Wnt pathway. It causes puckering of the skin and gradual flexion, usually of the ring and little fingers. It is more common in males, Caucasians, in diabetes mellitus and in those who overuse alcohol. A similar fibrosis occurs in the feet and is often more aggressive. It is also associated with Peyronie’s disease of the penis – a painful inflammatory disorder of the corpora cavernosa, leading eventually to painless fibrosis and angulation of the penis during erection. Intralesional steroid injections may help in early disease and some advocate transcutaneous needle aponeurotomy. Collagenase injection into the collagen contracted cord improved the amount of movement in one randomized study. Plastic surgical release of the contracture is restricted to those with severe deformity of the fingers.
Pain in the lower back
Low back pain is a common symptom. It is often traumatic and work-related, although lifting apparatus and other mechanical devices and improved office seating help to avoid it. Episodes are generally short-lived and self-limiting, and patients attend a physiotherapist or osteopath more often than a doctor. Chronic back pain is the cause of 14% of long-term disability in the UK. The causes are listed in Table 11.7, and the management of back pain is summarized in Box 11.2.
Table 11.7 Pain in the back (lumbar region): causes
Mechanical |
|
Postural back pain (sway back) Spinal and root canal stenosis Disseminated idiopathic skeletal hyperostosis (DISH) Fibromyalgia, chronic widespread pain (see p. 509) |
Inflammatory |
Metabolic |
Neoplastic (see p. 589) |
Referred pain |
Box 11.2
Management of back pain
Most back pain presenting to a primary care physician needs no investigation.
Pain between the ages of 20 and 55 years is likely to be mechanical and is managed with analgesia, brief rest if necessary and physiotherapy.
Patients should stay active within the limits of their pain.
Early treatment of the acute episode, advice and exercise programmes reduce long-term problems and prevent chronic pain syndromes.
Physical manipulation of uncomplicated back pain produces short-term relief and enjoys high patient satisfaction ratings.
Psychological and social factors may influence the time of presentation.
Investigations
Spinal X-rays are required only if the pain is associated with certain ‘red flag’ symptoms or signs, which indicate a high risk of more serious underlying problems:
MRI is preferable to CT scanning when neurological signs and symptoms are present. CT scans demonstrate bony pathology better. Interpretation of the relevance of the findings may require a specialist opinion.

Spinal metastasis in L2. The patient had severe back pain and weight loss and prior carcinoma of the breast.
Bone scans are useful in infective and malignant lesions but are also positive in degenerative lesions.
Full blood count, ESR and biochemical tests are required only when the pain is likely to be due to malignancy, infection or a metabolic cause. Normal ESR and CRP distinguish mechanical back pain from polymyalgia rheumatica, a likely differential in the elderly.
Mechanical low back pain
Mechanical low back pain starts suddenly, may be recurrent and is helped by rest. It is often precipitated by an injury and may be unilateral or bilateral. It is usually short-lived.
Examination and management
The back is stiff and a scoliosis may be present when the patient is standing. Muscular spasm is visible and palpable and causes local pain and tenderness. It lessens when sitting or lying. Pain relief and physiotherapy are helpful. Acupuncture helps some. Excessive rest should be avoided. Re-education in lifting and exercises help to prevent recurrent attacks of pain. Once a patient develops low back pain, although the episode itself is usually self-limiting, there is a significantly increased risk of further back pain episodes. Risk factors for recurrent back pain include:
pre-existing chronic widespread pain (fibromyalgia)
psychosocial factors such as high levels of psychological distress, poor self-rated health and dissatisfaction with employment.
Chronic low back pain is a major cause of disability and time off work and is reduced by appropriate early management.
Spinal movement occurs at the disc and the posterior facet joints, and stability is normally achieved by a complex mechanism of spinal ligaments and muscles. Any of these structures may be a source of pain. An exact anatomical diagnosis is difficult, but some typical syndromes are recognized (see below). They are often associated with but not necessarily caused by radiological spondylosis (see p.1148).
Postural back pain develops in individuals who sit in poorly designed, unsupportive chairs.
Lumbar spondylosis. The fundamental lesion in spondylosis occurs in an intervertebral disc, a fibrous joint whose tough capsule inserts into the rim of the adjacent vertebrae. This capsule encloses a fibrous outer zone and a gel-like inner zone. The disc allows rotation and bending.
Changes in the discs occasionally start in teenage years or early 20s and often increase with age. The gel changes chemically, breaks up, shrinks and loses its compliance. The surrounding fibrous zones develop circumferential or radial fissures. In the majority this is initially asymptomatic but visible on MRI as decreased hydration. Later the discs become thinner and less compliant. These changes cause circumferential bulging of the intervertebral ligaments.
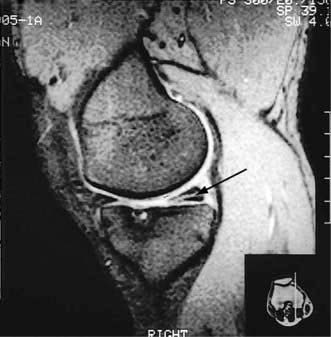
Reactive changes develop in adjacent vertebrae; the bone becomes sclerotic and osteophytes form around the rim of the vertebra (Fig. 11.6). The most common sites of lumbar spondylosis are L5/S1 and L4/L5.

Figure 11.6 MRI of lumbar spine, showing a central disc prolapse at the L4/L5 level (arrow). The signal from the L4/L5 and L5/S1 discs indicates dehydration, while the L3/L4 signal appearance is normal.
In young people, disc prolapse through an adjacent vertebral endplate produces a Schmorl’s node on X-ray. This is painless but may accelerate disc degeneration.
Spondylosis may be symptomless, but it can cause:
Facet joint syndrome. Lumbar spondylosis also causes secondary osteoarthritis of the misaligned facet joints. Pain is typically worse on bending backwards and when straightening from flexion. It is lumbar in site, unilateral or bilateral and radiates to the buttock. The facet joints are well seen on MRI and may show osteoarthritis, an effusion or a ganglion cyst. Direct corticosteroid injections into the joints under imaging may help but their long-term value is unclear. Physiotherapy to reduce hyperlordosis and reducing weight are helpful.
Fibrositic nodulosis. This causes unilateral or bilateral low back and buttock pain. There are tender nodules in the upper buttock and along the iliac crest. Such nodules are relevant only if they are tender. They are probably traumatic. Local, intralesional corticosteroid injections help.
Postural back pain and sway back of pregnancy. Low back pain is common in pregnancy and reflects altered spinal posture and increased ligamentous laxity. There is usually a hyperlordosis on examining the patient standing. Weight control and pre- and postnatal exercises are helpful, and the pain usually settles after delivery. Analgesics and NSAIDs are best avoided during pregnancy and breast-feeding. Epidurals during delivery are not associated with an increased incidence of subsequent back pain. Poor posture causes a similar syndrome in the non-pregnant, owing to obesity or muscular weakness. Poor sitting posture at work is a frequent cause of chronic low back pain.
Treatment of mechanical back pain
Adequate analgesia to allow normal mobility and avoid bed rest is best, combined with physical treatments such as physiotherapy, back muscle training regimens and manipulation. Manipulation produces more rapid pain relief in some patients. Acupuncture may help. Most episodes recover irrespective of the treatment given. A positive approach probably reduces the development of chronic pain. A comfortable sleeping position should be adopted using a mattress of medium (not hard) firmness.
Acute lumbar disc prolapse
The central disc gel may extrude into a fissure in the surrounding fibrous zone and cause acute pain and muscle spasm. These events are often self-limiting. A disc prolapse occurs when the extrusion extends beyond the limits of the fibrous zone (Fig. 11.6). The weakest point is posterolateral, where the disc may impinge on emerging spinal nerve roots in the root canal.
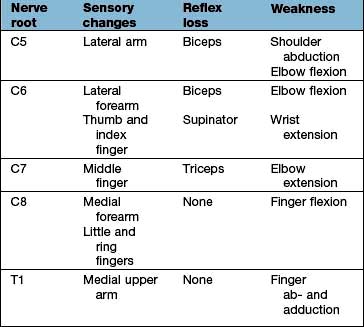
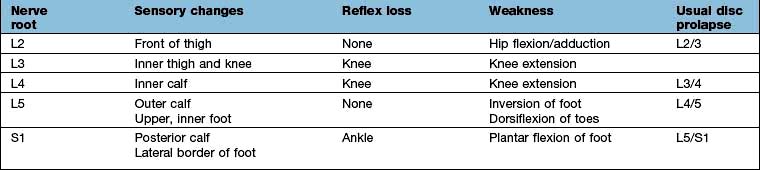
The episode often starts dramatically during lifting, twisting or bending and produces a typical combination of low back pain and muscle spasm, and severe, lancinating pains, paraesthesia, numbness and neurological signs in one leg (rarely both). The back pain is diffuse, usually unilateral and radiates into the buttock. The muscle spasm leads to a scoliosis that reduces when lying down. The nerve root pain develops with, or soon after, the onset. The site of the pain and other symptoms is determined by the root affected (Table 11.8). A central high lumbar disc prolapse may cause spinal cord compression and long tract signs (i.e. upper motor neurone). Below L2/L3 it produces lower motor neurone lesions.
On examination, the back often shows a marked scoliosis and muscle spasm. The straight-leg-raising test, whilst lying, is positive in a lower lumbar disc prolapse – raising the straight leg beyond 30° produces pain in the leg. Slight limitation or pain in the back limiting this movement is seen with mechanical back pain. Pain in the affected leg produced by a straight raise of the other leg suggests a large or central disc prolapse. Look for perianal sensory loss and urinary retention, which indicate a cauda equina lesion – a neurosurgical emergency (see p. 1135). An upper lumbar disc prolapse produces a positive femoral stretch test; pain in the anterior thigh when the knee is flexed in the prone position.
Treatment
Advise a short period (2–3 days) of bed rest, lying flat for a lower disc but semi-reclining for a high lumbar disc, and prescribe analgesia and muscle relaxants. Once the pain is tolerable, encourage the patient to mobilize and refer to a physiotherapist for exercises and preventative advice. An imaging-guided epidural or nerve root canal injection reduces pain rapidly, although the evidence that it speeds resolution or prevents surgery is unclear. Caudal epidural injections are less effective than lumbar ones. Resuscitation equipment must be available for these procedures. Referral to a surgeon for possible microdiscectomy or hemilaminectomy is necessary if the neurological signs are severe, if the pain persists and is severe for more than 6–10 weeks, or if the disc is central. If bladder or anal sphincter tone is affected it becomes a neurosurgical emergency.
Spinal and root canal stenosis
Progressive loss of disc height, OA of the facet joints, posterolateral osteophytes and buckling of the ligamentum flavum all contribute to root canal stenosis. This causes nerve root pain or spinal root claudication – pain and paraesthesiae in a root distribution brought on by walking and relieved slowly by rest. The associated sensory symptoms, slower recovery when the patient rests, and presence of normal foot pulses distinguish this from peripheral arterial claudication. Severe cervical spondylosis may also produce spinal claudication, often with arm symptoms and signs.
Spinal canal stenosis at more than one level is often associated with severe spondylosis and/or a congenitally narrow spinal canal. It causes buttock and bilateral leg pain, ‘heaviness’, paraesthesiae and numbness when walking. Rest helps, as does bending forwards, a manoeuvre that opens the spinal canal. Specialist surgical advice is necessary.
Spondylolisthesis
This occurs in adolescents and young adults when bilateral congenital pars interarticularis defects cause instability and permit a vertebra to slip, with or without preceding injury. Rarely, a cauda equina syndrome with loss of bladder and anal sphincter control and saddle-distribution anaesthesia develops. It is diagnosed radiologically. Low back pain in adolescents warrants investigation, and spondylolisthesis requires orthopaedic assessment. It needs careful monitoring during the growth spurt.
A degenerative spondylolisthesis may also develop in older people with lumbar spondylosis and osteoarthritis of the facet joints.
Diffuse idiopathic skeletal hyperostosis (DISH)
DISH (Forestier’s disease) affects the spine and extraspinal locations. It causes bony overgrowths and ligamentous ossification and is characterized by flowing calcification over the anterolateral aspects of the vertebrae. The spine is stiff but not always painful, despite the dramatic X-ray changes. Ossification at muscle insertions around the pelvis produces radiological ‘whiskering’. Similar changes occur at the patella and in the feet. It is commoner in people with metabolic syndrome (high BMI, diabetes mellitus, hypertension and dyslipidaemia; see p. 1006).
Treatment is with analgesics or NSAIDs for pain, and exercise to retain movement and muscle strength.
Osteoporotic crush fracture of the spine
Osteoporosis is asymptomatic but leads to an increased risk of fracture of peripheral bones, particularly neck of femur and wrist, and thoracic or lumbar vertebral crush fractures. Such vertebral fractures develop without trauma, after minimal trauma, or as part of a major accident. They may develop painlessly or cause agonizing localized pain that radiates around the ribs and abdomen. Multiple fractures lead to an increased thoracic kyphosis (‘widow’s stoop’). They cause disability and reduced QoL. The diagnosis is confirmed by X-rays, showing loss of anterior vertebral body height and wedging, with sparing of the vertebral endplates and pedicles. Bone oedema on MRI indicates that a fracture is recent. An underlying tumour and pathological fracture need to be excluded.
Treatment
Advise bed rest and analgesia until the severe pain subsides over a few weeks, then gradual mobilization. It may warrant hospitalization, and intravenous bisphosphonates or subcutaneous or nasal calcitonin are given to relieve pain. There may be some residual pain and deformity.
The role of percutaneous vertebroplasty and balloon kyphoplasty remains unclear: there are no randomized controlled trials showing any benefit. Both involve inserting a needle through a pedicle into the affected vertebral body under CT guidance with the aim of stabilizing the fracture. Kyphoplasty involves inflating a balloon filled with methyl methacrylate cement in order to restore vertebral shape. Vertebroplasty is the injection of cement alone, without restoring vertebral shape. Pain relief is usual with both but the risks are higher with vertebroplasty. Deciding when to intervene is complicated by the spontaneous recovery that many experience.
Bone density measurement and preventative treatment of osteoporosis are essential (see p. 555).
Septic discitis may cause severe pain and rapid adjacent vertebral destruction. It is seen on MRI and requires urgent neurosurgical referral.
Ankylosing spondylitis (see p. 527)
Buttock pain and low back stiffness in a young adult suggests ankylosing spondylitis, especially if it is worse at night and in the morning.
Pain in the hip (table 11.9)
‘Hip’ refers to a wide area between the upper buttock, trochanter and groin. It is useful to ask the patient to point to the site of pain and its field of radiation. Pain arising from the hip joint itself is felt in the groin, lower buttock and anterior thigh, and may radiate to the knee. Occasionally and inexplicably, hip arthritis causes pain only in the knee.
Table 11.9 Pain in the hip: causes
| Hip region problems | Main sites of pain |
|---|---|
Osteoarthritis of hip |
Groin, buttock, front of thigh to knee |
Trochanteric bursitis (or gluteus medius tendonopathy) |
Lateral thigh to knee |
Meralgia paraesthetica |
Anterolateral thigh to knee |
Referred from back |
Buttock |
Facet joint pain |
Buttock and posterior thigh |
Fracture of neck of femur |
Groin and buttock |
Inflammatory arthritis |
Groin, buttock, front of thigh to knee |
Sacroiliitis (AS) |
Buttock(s) |
Avascular necrosis |
Groin and buttocks |
Polymyalgia rheumatica |
Lumbar spine, buttocks and thighs |
AS, ankylosing spondylitis.
Osteoarthritis (OA)
OA (see p. 512) is the most common cause of hip joint pain in a person over the age of 50 years. It causes pain in the buttock and groin on standing and walking. Stiff hip movements cause difficulty in putting on a sock and may produce a limp. Sudden onset pain may be associated with an effusion on MRI and can be treated by an ultrasound guided steroid injection.
Lateral hip pain syndrome: trochanteric bursitis and gluteus medius tendonopathy
This may be due to trochanteric bursitis and caused by trauma or unaccustomed exercise. It also occurs in inflammatory arthritis. The pain over the trochanter is worse going up stairs, and the trochanter is tender to lie on. Its best management is unclear but exercises help, as may a local corticosteroid injection, although the evidence base for treatment is poor. Surgery is occasionally necessary. Lateral hip pain may be referred from the upper lumbar spine. A tear of the gluteus medius tendon at its insertion into the trochanter causes a similar syndrome but does not respond to injection. MRI scans have demonstrated this new syndrome.
Meralgia paraesthetica
This causes numbness and burning dysaesthesia (increased sensitivity to light touch) over the anterolateral thigh and may be precipitated by a sudden increase in weight, an injury or during pelvic surgery. It is usually self-limiting but can be helped by amitriptyline or gabapentin at night.
Fracture of the femoral neck
This usually occurs after a fall, occasionally spontaneously. There is pain in the groin and thigh, weight-bearing is painful or impossible, and the leg is shortened and externally rotated. Occasionally, a fracture is not displaced and remains undetected. X-rays are diagnostic. Anyone with a hip fracture, especially after minimal trauma, should be reviewed for osteoporosis (see p. 553).
Avascular necrosis (osteonecrosis) of the femoral head
This is uncommon but occurs at any age. (Risk factors are discussed on p. 556.) There is severe hip pain. X-rays are diagnostic after a few weeks, when a well-demarcated area of increased bone density is visible at the upper pole of the femoral head. The affected bone may collapse. Early, the X-ray is normal but bone scintigraphy or MRI demonstrates the lesion and shows bone marrow oedema.
Inflammatory arthritis of the hip
This produces pain in the groin and stiffness, which are worse in the morning. Rheumatoid arthritis (RA) rarely presents with hip pain, although the hip is involved eventually in severe RA. Ankylosing spondylitis and other seronegative spondyloarthropathies cause inflammatory hip arthritis in younger people.
Polymyalgia rheumatica
Bilateral hip, buttock and thigh pain and stiffness that are worse in the morning in an elderly patient may be attributable to polymyalgia rheumatica (see p. 542). Neck and shoulder pain and stiffness are usually also present.
Pain in the knee (table 11.10)
The knee depends on ligaments and quadriceps muscle strength for stability. It is frequently injured, particularly during sports. Trauma or overuse of the knee leads to a variety of peri- and intra-articular problems. Some are self-limiting; others require physiotherapy, local corticosteroid injections or surgery.
Trauma and overuse |
Periarticular problems |
Osteoarthritis/Inflammatory arthritis |
Other |
The knee is also a common site of inflammatory arthritis and osteoarthritis. Minor radiographic changes of osteoarthritis (see Fig. 11.11) are common in the over-50s and often coincidental, the cause of the pain being periarticular. Symptomatic osteoarthritis of the knee correlates poorly with the severity of the radiological changes.
Common periarticular knee lesions
There may be medial or lateral ligament strain, but the medial ligament is more commonly affected. There is pain at the ligament’s insertion into the upper medial tibia, which is worsened by standing or stressing the affected ligament.
Anserine bursitis causes pain and localized tenderness 2–3 cm below the posteromedial joint line in the upper part of the tibia at the site of the bursa. It occurs in obese women, often with valgus deformities, and in breast-stroke swimmers.
Treatment is with physiotherapy and a local corticosteroid injection.
Anterior knee pain is common in adolescence. In many cases, no specific cause is found, despite investigation. This is called ‘anterior knee pain syndrome’ and settles with time. Isometric quadriceps exercises and avoidance of high heels both help the condition. Patient and parents often need firm reassurance. Abnormal patellar tracking may be a cause and need surgical treatment. Hypermobility of joints causes joint pain, maltracking and rarely recurrent patellar dislocation (see also p. 546).
Pre- and infrapatellar bursitis are caused by unaccustomed kneeling (‘housemaid’s knee’). There is local pain, tenderness and fluctuant swelling. Avoidance of kneeling and a local corticosteroid injection are helpful. Septic bursitis can occur.
Osgood–Schlatter disease (p. 546) causes pain and swelling over the tibial tubercle. It is a traction apophysitis of the patellar tendon and occurs in enthusiastic teenage sports players.
Enthesitis may occur at the patellar end of the tendon (jumper’s knee).
Common intra-articular traumatic lesions of the knee
This is diagnosed arthroscopically. The retropatellar cartilage is fibrillated. In most cases the pain settles eventually. When there is patellar misalignment it may need surgery, as does recurrent patellar dislocation in adolescent girls.
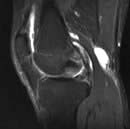
The menisci are partially attached fibrocartilages that stabilize the rounded femoral condyles on the flat tibial plateaux. In the young they are resilient but this decreases with age. They can be torn by an injury, commonly in sports that involve twisting and bending. The history is usually diagnostic. There is immediate medial or lateral knee pain and swelling within a few hours. The affected side is tender. If the tear is large the knee may lock flexed. The immediate treatment is to apply ice. MRI demonstrates the tear (Fig. 11.7). In most circumstances, especially in active sportsmen, early arthroscopic repair or trimming of the torn meniscus is essential. Surgical intervention reduces recurrent pain, swelling and locking but not the risk of secondary osteoarthritis. The long-term benefit of early repair of tears is not yet known. Post-surgical quadriceps exercises aid a return to sport and other activities.
Torn cruciate ligaments account for around 70% of knee haemarthroses in young people. They often co-exist with a meniscal tear. Partial cruciate tears are difficult to diagnose clinically. On flexing the knee to 90°, a torn anterior cruciate allows the tibia to be pulled forwards on the femur. MRI is the investigation of choice. Such injuries need urgent orthopaedic referral, reconstructive surgery usually being necessary in young active adults. There is a significant incidence of secondary OA.
This occasionally causes knee pain and swelling in adolescents and young adults, more commonly males. It is probably traumatic, possibly with hereditary predisposing factors. A fragment of bone and its attached cartilage detach by shearing, most commonly from the lateral aspect of the medial femoral condyle.
There is aching pain after activity and, if the fragment becomes loose, locking or ‘giving way’ occurs. The lesion is seen on a tunnel-view X-ray, but MRI is more sensitive, especially if the fragment is undisplaced. Undisplaced lesions are treated with rest, then isometric quadriceps exercises. Loose fragments can be fixed arthroscopically or removed. A similar lesion affecting the lateral femoral condyle occurs in older people.
Spontaneous osteonecrosis of the knee (SONK)
This may occur spontaneously or after injury. There is local pain and there are marked bone marrow changes on MRI or SPECT-CT. Weight-bearing must be avoided. Pamidronate by infusion is sometimes used. It may progress to bone infarction and require replacement surgery.
Spontaneous osteonecrosis of the knee. MRI showing a high signal in the posterior aspect of the femoral condyle, a small effusion and a popliteal cyst.

Spontaneous osteonecrosis of the knee. SPECT-CT showing a high signal in the posterior medial femoral condyle.
Occasionally, spontaneously or after trauma, osteonecrosis of the knee is associated with severe pain and striking findings on MRI, which is often called SONK (spontaneous osteonecrosis of the knee).
Knee joint effusions
An effusion of the knee causes swelling, stiffness and pain. The pain is more severe with an acute onset and with increasing inflammation, because of stretching of the capsule that contains the pain receptors. A full clinical history must include a past medical, family and drug history.
Inflammatory arthritis affects the knees and causes warmth and swelling. An acute inflammatory monoarthritis of the knee is a common presentation of a spondyloarthritis and occasionally is the first sign of RA.
Monoarthritis of the knee, associated with severe pain and marked redness, may be due to septic arthritis, or gout in the middle-aged male, or to gout or pseudogout in an older male or female. A cool, clear, viscous effusion is seen in elderly people with moderate or severe symptomatic OA (see p. 512).
Examination
A large and tense effusion is easily seen and felt on each side of the patella and in the suprapatellar pouch, and is fluctuant. The effusion delays the patella tapping against the femur when it is pressed firmly and quickly (the ‘patellar tap’ sign) with the knee held straight and relaxed. Small effusions also demonstrate the ‘bulge’ sign when the patient is lying with the quadriceps relaxed. For this, apply a gentle sweeping pressure, first to the medial side of the joint and then, watching the medial dimple, to the lateral side. Slightly delayed bulging of the medial dimple indicates fluid in the joint.
Investigations
These are (a) blood tests, and (b) aspiration (Fig. 11.8) and examination of the knee effusion. The basic technique of aspiration is described in Practical Box 11.2.

Practical Box 11.2 Joint aspiration
This is a sterile procedure which should be carried out in a clean environment
Explain the procedure to the patient; obtain consent.
1. Decide on the site to insert the needle and mark it.
2. Clean the skin and your hands scrupulously; remove rings and wristwatch. Put on gloves.
3. Draw up local anaesthetic (and corticosteroid if it is being used) and then use a new needle.
4. Warn the patient, insert the needle, injecting local anaesthetic as it advances and, if a joint effusion is suspected, attempt to aspirate as you advance it.
5. If fluid is obtained, change syringes and aspirate fully.
6. Examine the fluid in the syringe and decide whether or not to proceed with a corticosteroid injection (if fluid clear or slightly cloudy) or send for microbiological tests.
7. Cover the injection site and advise the patient to rest the affected area for a few days. Warn the patient that the pain may increase initially but to report urgently if this persists beyond a few days, if the swelling worsens, or if they become febrile, since this might indicate an infected joint.
Trauma: meniscal, cruciate or synovial lining tear
Clotting or bleeding disorders: such as haemophilia, sickle cell disease or von Willebrand’s disease.
Popliteal cyst (Baker’s cyst). In approximately 5% of people with a knee effusion, a swollen, painful popliteal cyst develops. The semimembranosus bursa in some individuals has a valve-like connection to the knee. This allows the effusion to flow into the bursa but not back. The cyst is best seen and felt in the popliteal fossa with the patient standing.
Ruptured popliteal cyst. A popliteal cyst may rupture if the patient is mobile. Fluid escapes into the soft tissue of the popliteal fossa and upper calf, causing sudden and severe pain, swelling and tenderness of the upper calf. Dependent oedema of the ankle develops and the knee effusion reduces dramatically in size and may be undetectable.
A history of previous knee problems and the sudden onset of pain and tenderness high in the calf suggest a ruptured cyst rather than a deep vein thrombosis (DVT). However, the diagnosis is often missed and treated inappropriately with anticoagulants. A diagnostic ultrasound examination distinguishes a ruptured cyst from a DVT (see p. 789). Analgesics or NSAIDs, rest with the leg elevated, and aspiration and injection with corticosteroids into the knee joint are required.
Pain in the foot and heel (table 11.11)
The feet are subjected to extreme pressures by weight-bearing and inappropriate shoes. They are commonly painful. Broad, deep, thick-soled shoes are essential for sporting activities, prolonged walking or standing, and in people with congenitally flat or arthritic feet.
Table 11.11 Pain in the foot and heel: causes
Structural (flat (pronated) or high arched (supinated)) |
|
Hallux valgus/rigidus (±OA) |
|
Metatarsalgia |
|
Morton’s neuroma |
|
Stress fracture |
|
Inflammatory arthritis |
|
Acute, monoarticular – gout |
|
Chronic, polyarticular – RA |
|
Chronic, pauciarticular – spondyloarthritis |
|
Tarsal tunnel syndrome |
|
Heel pain |
|
Plantar fasciitis |
Below heel |
Plantar spur |
Below heel |
Achilles tendonitis/bursitis |
Behind heel |
Sever’s disease |
Behind heel |
Arthritis of ankle/subtaloid joints |
|
There are two common types of foot deformity:
Flat feet: stress the ankle and throw the hindfoot into a valgus (everted) position. A flat foot is rigid and inflexible.
High-arched feet: place pressure on the lateral border and ball of the foot.
The foot is affected by a variety of inflammatory arthritic conditions. After the hand, the foot joints are the most commonly affected by rheumatoid arthritis. The diagnosis depends upon careful assessment of the distribution of the joints affected, the pattern of other joint problems or by finding the associated condition (e.g. psoriasis, see p. 1207).
The great toe migrates laterally. In the congenital form, the first metatarsal bone is displaced medially (metatarsus primus varus). The shape of modern shoes causes later onset of hallux valgus. It is a common complication of RA.
Osteoarthritis of the first metatarsophalangeal (MTP) joint in a normally aligned or valgus joint causes hallux rigidus: a stiff, dorsiflexed and painful great toe. Careful choice of footwear and the help of a podiatrist suffice for most cases, but some require surgery.
This is common, especially in women who wear high heels, after trauma and in those with hammer toes. The ball of the foot is painful to walk and stand on. Callosities and pressure- induced bursae develop under the metatarsal heads. Rheumatoid arthritis causes misalignment of the metatarsal bones and severe metatarsalgia.
Treatment is with podiatry and the wearing of appropriate shoes. Surgery is occasionally needed, particularly in the rheumatoid forefoot.
Morton’s metatarsalgia is due to a neuroma, usually between the third and fourth metatarsal heads. It causes pain, burning and numbness in the adjacent surfaces of the affected toes when walking. It is helped by wearing wider, cushioned-soled shoes. Occasionally a steroid injection or excision is necessary.
These cause sudden, severe, weight-bearing pain in the distal shaft of the fractured metatarsal bone. They occur after unaccustomed walking or with new shoes. There is local tenderness and swelling, but initially X-rays are normal and diagnosis delayed. A radioisotope bone scan or MRI reveals the fracture earlier than X-rays. Reduced weight-bearing for a few weeks usually suffices. There is a possibility of osteoporosis.

This is an entrapment neuropathy of the posterior tibial nerve at the medial malleolus. It produces burning, tingling and numbness of the toes, sole and medial arch. The nerve is tender below the malleolus and, when tapped, produces a shock-like pain (Tinel’s sign). A local steroid injection under the retinaculum, between the medial malleolus and calcaneum, is helpful.
Plantar fasciitis is an enthesitis at the insertion of the tendon into the calcaneum. It produces localized pain under the heel when standing and walking, and local tenderness. It occurs alone or in spondyloarthritis.
Plantar spurs are traction lesions at the insertion of the plantar fascia in older people and are usually asymptomatic. They become painful after trauma.
Calcaneal bursitis is a pressure-induced (adventitious) bursa that produces diffuse pain and tenderness under the heel. Compression of the heel pad from the sides is painful, which distinguishes it from plantar fascia pain.
Whatever the cause, the pain is always worse in the morning as soon as weight is placed on the foot.
All of these lesions are treated with heel pads, and reduced walking; they are often self-limiting. A dorsiflexion splint at night to stretch the plantar fascia is worth trying. When an injection is necessary, a medial approach is used, rather than through the heel pad, often under ultrasound guidance.
Sever’s disease is a traction apophysitis of the Achilles tendon in young people (cf. Osgood–Schlatter disease, p. 546).
Pain at the insertion of the Achilles tendon into the calcaneum is an enthesitis. This is traumatic or it can complicate spondyloarthritis. Raising the shoe heel reduces pain. Occasionally a low-pressure corticosteroid injection near the enthesis is necessary.
Achilles tendonosis causes a painful, tender swelling a few centimetres above the tendon’s insertion. Advise against walking barefoot and jumping. Tendon damage or rupture can occur with quinolone, e.g. ciprofloxacin therapy. Therapeutic ultrasound is helpful. (Caution: a local injection may cause the tendon to rupture.) Autologous platelet concentrates are used but evidence for efficacy is poor.
Achilles bursitis lies clearly anterior to the tendon and can be safely injected with corticosteroid.
The muscles of the lower leg are enclosed in fascial compartments, with little room for expansion to occur. Compartment syndromes can be acute and severe, such as following exercise.
In the anterior tibial syndrome there is severe pain in the front of the shin, occasionally with foot drop. Immediate surgical decompression to prevent muscle necrosis is sometimes required.
Chronic compartment syndrome produces pain in the lower leg that is aggravated by exercise and may therefore be mistaken for a vascular or neurological disorder.
Pain in the chest
Musculoskeletal conditions are sometimes a cause of chest pain. An example is Tietze’s disease. In this condition, pain arises from the costosternal junctions. It is usually unilateral and affects one, two or three ribs. There is local tenderness, which helps to make the diagnosis. The condition is benign and self-limiting. It often responds well to anti-inflammatory drugs. Other causes of chest wall pain include rib fractures due to trauma or osteoporosis or a malignant deposit. Costochondral pain occurs in ankylosing spondylitis (see p. 527). In people with heart disease, costochondral pain may cause severe anxiety but it is not like angina and the patient should be reassured.
Chronic pain syndromes
Chronic pain syndromes (see p. 1163) are difficult to manage. Psychological factors are at least as relevant as inflammation or damage in determining the patient’s perception of pain. It is essential to be objective and non-judgemental when discussing physical, psychological and social factors without assuming which is primary. Chronic pain syndromes are difficult to explain scientifically. It is all too easy for a doctor to respond to this lack of a clear scientific cause by seeming to ‘blame’ the patient for the symptoms. Many chronic pain states are post-traumatic and some may be exacerbated partly by the process of litigation that may follow an injury.
Any chronic painful condition can change the way a person copes. Some people with chronic diseases or chronic pain cope well, but others adopt coping strategies and patterns of behaviour which make things worse. They become anxious, depressed or socially isolated, and their QoL is reduced. In chronic pain syndromes patients need help to lead a more normal life despite their pain, and are best referred to a specialist, multidisciplinary pain service.
Psychological states such as depression and anxiety produce physical symptoms, of which one is pain, while people with frank physical diseases are often understandably anxious and depressed. A biopsychosocial approach is best.
Chronic widespread pain (fibromyalgia)
Chronic widespread pain is defined as pain for more than three months both above and below the waist (p. 1163). It is a diagnosis of exclusion although it is still not universally accepted as a diagnosis. Multiple trigger points are reported by people with fibromyalgia (see p. 1163; Fig. 11.9). The pain is widespread, with unremitting, aching discomfort. Many patients have sleep disturbances, so they awake unrefreshed and have poor concentration. Multiple other symptoms, e.g. irritable bowel syndrome (IBS), tension headaches, dysmenorrhoea, atypical facial or chest pain, often co-exist. It occurs at any age and affects women more than men (7:1).
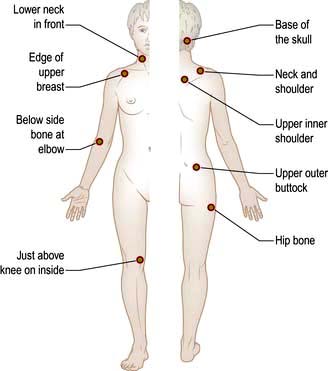
Doctors sometimes inappropriately label these patients ‘heart sink’ patients and patients sense this. The patient’s frustration is compounded by the fact that most tests are normal, and they fear doctors believe it is ‘all in their mind’. Sleep disturbance may lead to abnormalities of serotonin, substance P and cortisol levels. This is best regarded as a ‘wind up’ or pain amplification syndrome and is attributable to changes in the descending inhibitory pathways and in the spinal cord, resulting in a maladaptive pain response.
Treatment (see p. 1163)
A sympathetic, psychosocial, multidisciplinary approach is appropriate. A graded, supervised aerobic exercise regimen over 3 months is safe and effective. When depression is present, it should be treated. Cognitive behavioural therapy can help the person to pace their life more effectively and to cope better, although patients often resist referral for psychological help.
analgesics (e.g. paracetamol or weak opioids), help, and pregabalin and antidepressant drugs, such as fluoxetine, help when depression is a major factor.
Low-dose amitriptyline or dosulepin help sleep disturbance when taken a few hours before bedtime. They act by increasing the levels of serotonin (5HT) in the CNS and probably increasing descending sensory inhibition. It should be explained that these doses are analgesic and not antidepressant, and their side-effects should be outlined.
Trigger-point injections with local anaesthetic, corticosteroids or acupuncture are sometimes helpful. Oral corticosteroids are not helpful.
Chronic fatigue syndrome
Diffuse muscular pain and stiffness is common in this condition, which is described on page 1162.
Chronic (work-related) upper-limb pain syndrome
This name is preferred to ‘repetitive strain injury’ (RSI). The predominant symptoms are pain in all or part of one or both arms. A specific lesion, such as tennis elbow or carpal tunnel syndrome, or muscular-pattern neck pain often develops first, and early recognition and treatment may prevent chronicity. After a variable period, the pain becomes more diffuse and no longer simply work-related, and there is often severe distress. It is seen in keyboard workers and in musicians. When it arises at work, it is often at a time of changing work practices, shortage of staff or disharmony. Middle managers find it difficult to deal with and this compounds the stress.
It is seen throughout the developed world. It peaked in incidence in Australia in the 1970s and 1980s but has largely disappeared there, apparently because of changes in work practices, improvements in early medical management, changes in workers’ compensation legislation, and reduced media discussion of the problem.
Treatment
If possible, there should be a brief period off work and a gradual return to activity as the pain settles. Use of analgesia and NSAIDs, with physiotherapy, is helpful during the initial phase to prevent a vicious circle developing. Amitriptyline or pregabalin is helpful for some patients.
A review of working practices and the positioning of screen, keyboard and chair are essential, as is support of the patient by their manager. Musicians are helped by expert advice on playing technique and should reduce playing times temporarily, but not stop completely.
Temporomandibular pain dysfunction syndrome
This is a disorder of the temporomandibular joint associated with nocturnal tooth grinding or abnormalities of bite. It occurs in anxious people. It gives rise to pain in one or both temporomandibular joints.
Dental correction of the bite helps a few but when no dental cause is found, low-dose tricyclic antidepressant therapy is used. Many patients are made worse by unnecessary dental treatment.
Hypermobility and hypermobility syndrome
Many people in the adult population have hypermobile joints (see p. 546). A small proportion are more prone to joint pains, joint instability and autonomic disturbances. This sometimes causes extreme anxiety and manifests as a chronic pain syndrome. Specific exercises to stabilize the joints, recognition of the problem and, sometimes, cognitive behavioral therapy all help. Surgery is best avoided because of problems with healing.
Chronic regional pain syndrome type I (previously called reflex sympathetic dystrophy or Sudeck’s atrophy)
This is defined as ‘a complex disorder or group of disorders that may develop as a consequence of trauma affecting the limbs, with or without obvious nerve lesions’. It may also develop after central nervous system lesions (e.g. strokes) or without cause. Its features are pain and other sensory abnormalities, including hyperaesthesia, autonomic vasomotor dysfunction, leading to abnormal blood flow and sweating, and motor system abnormalities. This leads to structural changes of superficial and deep tissues (trophic changes). Not all components need be present. The sensory, motor and sympathetic nerve changes are not restricted to the distribution of a single nerve and may be remote from the site of injury. The early phase, with pain, swelling and increased skin temperature, is difficult to diagnose but potentially reversible.
After a period of weeks or months, a second, still painful, dystrophic phase develops, characterized by articular stiffness, cold skin and trophic changes, often with localized osteoporosis.
A late phase involves continued pain, skin and muscle atrophy, and muscle contractures, and is extremely disabling.
Diagnosis is initially clinical – a high index of suspicion and recognizing the unusual distribution of the pain. A three-phase bone scan shows diffuse or patchy increase in uptake in the affected limb in all three phases. MRI also shows these early changes. Demineralization on X-ray occurs later.
Treatment
Management is difficult and the problem often very disabling. The evidence base for treatment is poor. Early diagnosis, effective pain relief and general care of the patient are essential. NSAIDs, corticosteroids and pregabalin or gabapentin are used in the early phase, together with active exercise of the limb encouraged by a physiotherapist. Intravenous disodium pamidronate can be used at this stage. Referral to a specialist pain clinic is essential. A stellate ganglion block may help upper limb involvement and a sympathetic chain block for the lower limb. Guanethidine (an alpha-blocking agent) or lidocaine administered to the limb under tourniquet are also used.
Analgesic and anti-inflammatory drugs for musculoskeletal problems
The key to using drugs, particularly in chronic disorders and the elderly, is to balance risk and benefit and constantly to review their appropriateness. Box 11.3 shows the main drugs available.
Box 11.3
Analgesics and NSAIDs
Analgesics (in order of potency) Advise that they be taken only if needed. Maximum doses are indicated here: |
||
Paracetamol |
500–1000 mg |
6-hourly |
Paracetamol (500 mg) and codeine (8–30 mg) |
1–2 tablets |
6-hourly |
Dihydrocodeine |
30–60 mg |
Every 6–8 h |
Paracetamol with dihydrocodeine |
1–2 tablets |
Every 6–8 h |
Non-steroidal anti-inflammatory drugs (NSAIDs) |
||
Always to be taken with food. Use slow-release preparations in inflammatory conditions or if more regular pain control is needed. Examples are: |
||
Ibuprofen |
200–400 mg |
Every 6–8 h |
Ibuprofen slow release |
600–800 mg |
12-hourly |
Diclofenac |
25–50 mg |
8-hourly |
Diclofenac slow release |
75–100 mg |
× 1–2 daily |
Naproxen |
250 mg |
× 3–4 daily |
Naproxen slow release |
550 mg |
× 2 daily |
Celecoxiba |
100–200 mg |
× 2 daily |
Simple and compound analgesic agents
Simple agents such as paracetamol, aspirin, or codeine compounds (or combination preparations), used when necessary or regularly, relieve pain and improve function. Sleep may also be improved. Side-effects are relatively infrequent, although drowsiness and constipation occur with codeine preparations, especially in the elderly.
Stronger analgesics, such as dihydrocodeine or morphine derivatives, should be used only with severe pain.
Non-steroidal anti-inflammatory drugs (NSAIDs)
NSAIDs have anti-inflammatory and centrally acting analgesic properties. They inhibit cyclo-oxygenase (COX), a key enzyme in the formation of prostaglandins, prostacyclins and thromboxanes (see Fig. 15.30). There are two specific cyclo-oxygenase enzymes:
COX-1 is the constitutive form present in many normal tissues.
COX-2 is the form mainly induced in response to pro-inflammatory cytokines and not found in most normal tissues (except the kidney). It is associated with oedema and the nociceptive and pyretic effects of inflammation.
Most of the older NSAIDs are nonspecific and block both enzymes but with variable specificity (‘nonspecific NSAIDs’ or nsNSAIDs). Their therapeutic effect depends on blocking COX-2 and their side-effects mainly on blocking COX-1. COX-1 protects the gastric mucosa and blocking it accounts for the majority of upper gastrointestinal side-effects.
The most common side-effects with nonspecific NSAIDs are indigestion or skin rashes. More serious upper gastrointestinal side-effects are gastric erosions and peptic ulceration with perforation and bleeding. These occur more frequently in the elderly, in whom mortality is higher, in long-term use, and in those with high risk factors: a history of ulcers, Helicobacter pylori, and concurrent corticosteroids or anticoagulant therapy. Ibuprofen, in combination with low-dose aspirin, significantly increases the risk of severe gastrointestinal bleeding. Practice guidelines recommend proton pump inhibitors in high-GI-risk patients on nonspecific NSAIDs. H2 blockers are less effective as gastroprotective agents. Prostaglandin E2 analogues, e.g. misoprostol, reduce ulcer complications and are popular but may cause nausea and diarrhoea. Lower gastrointestinal (GI) side-effects of nonspecific NSAIDs are becoming more common.
COX-2 inhibitors (‘Coxibs’) produce fewer gastrointestinal side-effects but they still occur. Coxibs are used in patients who have a high risk of gastrointestinal disease and with no cardiovascular risk. People with a high risk of both may be better off taking an NSAID (ibuprofen or naproxen) or a Coxib with a proton pump inhibitor.
Coxibs and NSAIDs may reduce renal function, especially in the elderly (see Box 12.3, p. 608) and rarely cause cardiovascular events.
Short courses of NSAIDs or coxibs are used in musculoskeletal pain and in osteoarthritis and spondylosis but simple analgesia is often more appropriate.
In crystal synovitis, NSAIDs and coxibs have a true anti-inflammatory effect (see p. 511).
In chronic inflammatory synovitis, NSAIDs and coxibs do not alter the chronic inflammatory process, or decrease the risk of joint damage, but they do reduce pain and stiffness.
Slow-release preparations are useful for inflammatory arthritis and when more constant pain control is needed.
Be aware of the patient’s gastrointestinal and cardiac risks before prescribing NSAIDs or coxibs.
Osteoarthritis (OA)
Osteoarthritis is the most common type of arthritis. It occurs with a variety of patterns in synovial joints and is characterized by cartilage loss with an accompanying periarticular bone response. It is probably not a single disease entity but a multifactorial process in which mechanical factors have a central role. The whole joint structure including cartilage, subchondral bone, ligaments, menisci, synovium and capsule is involved. Pathologically, there is significant inflammation of articular and periarticular structures and alteration in cartilage structure. Osteoarthritis is the subject of intense investigation but no drugs which halt or reverse this process have yet been developed.
Epidemiology
The prevalence of OA increases with age; it is uncommon below the age of 50 years and most people over 60 years will have some radiological evidence of it, although only a quarter of these will be symptomatic. It occurs worldwide, but with a variable distribution, e.g. in Asians, hip OA is less common and knee OA is more common than in Europeans. Women over 55 years are affected more commonly than men of a similar age. There is a familial pattern of inheritance in nodal OA and in primary generalized OA. OA has a variable distribution (Fig. 11.10). The resulting disabilities have major socioeconomic resource implications, particularly in the developed world. OA is the most common cause of disability in the Western world in older adults.
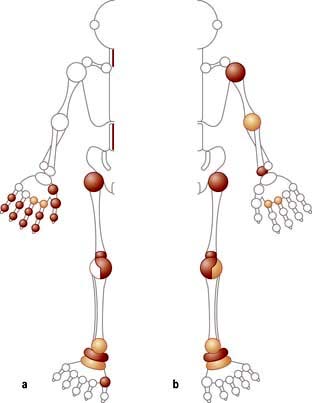
Aetiology (Box 11.4)
The gene that encodes collagen type II (COL2A1) is a candidate gene for familial OA but there is no single gene that associates with all patterns of OA. Abnormal local mechanical factors which affect loading and wear, such as prior injury, instability, hypermobility and joint dysplasia, play a role in most types of OA. Inflammation starting at periarticular entheses is seen during the inflammatory phase on MRI in nodal OA. Osteoarthritis is the result of active, sometimes inflammatory but potentially reparative processes rather than the inevitable result of trauma and ageing. Focal destruction of the articular cartilage is the common pathological feature. The spectrum of OA ranges from atrophic disease in which cartilage destruction occurs without any subchondral bone response, to hypertrophic disease in which there is massive new bone formation at the joint margins.
Box 11.4
Factors predisposing to osteoarthritis
Obesity: Predicts later risk of radiological and symptomatic OA of the hip and hand in population studies
Heredity: Familial tendency to develop nodal and generalized OA
Gender: Polyarticular OA is more common in women; a higher prevalence after the menopause suggests a role for sex hormones
Hypermobility (see p. 546): Increased range of joint motion and reduced stability lead to OA
Osteoporosis: There is a reduced risk of OA
Diseases: See Table 11.12
Trauma: A fracture through any joint. Meniscal and cruciate ligament tears cause OA of the knee
Congenital joint dysplasia: Alters joint biomechanics and leads to OA. Mild acetabular dysplasia is common and leads to earlier onset of hip OA
Joint congruity: Congenital dislocation of the hip or a slipped femoral epiphysis or Perthes’ disease; osteonecrosis of the femoral head (see p. 556) in children and adolescents causes early-onset OA
Occupation: Miners develop OA of the hip, knee and shoulder, cotton workers OA of the hand, and farmers OA of the hip
Sport: Repetitive use and injury in some sports causes a high incidence of lower-limb OA.
Cartilage is a matrix of collagen fibres, which enclose a mixture of proteoglycans and water (see p. 494). The gene for human aggrecan has been cloned, and polymorphisms of the gene have been correlated with OA of the hand in older men.
Cartilage is smooth-surfaced and shock-absorbing. Under normal circumstances, there is a dynamic balance between cartilage degradation by wear and its production by chondrocytes. Early in the development of OA, this balance is lost and, despite increased synthesis of extracellular matrix, the cartilage becomes oedematous. Focal erosion of cartilage develops. Chondrocytes die and, although repair is attempted from adjacent cartilage, the process is disordered. Eventually the synthesis of extracellular matrix fails and the surface becomes fibrillated and fissured. Cartilage ulceration exposes underlying bone to increased stress, producing microfractures and cysts. The bone attempts repair but produces abnormal sclerotic subchondral bone and overgrowths at the joint margins, called osteophytes (Fig. 11.11). There is some secondary inflammation.
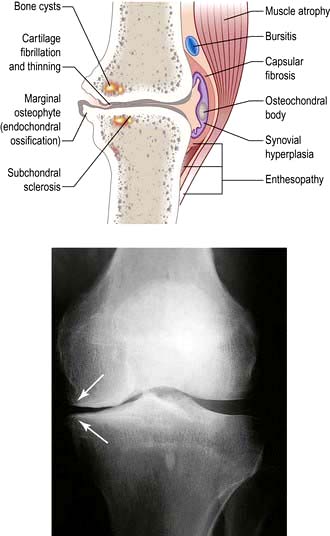
Pathogenesis
Several mechanisms have been suggested:
Abnormal stress and loading leading to mechanical cartilage damage play a role in secondary OA.
Obesity is a risk factor for developing OA of the hand and knee, but not the hip in later life. Increased skeletal mass increases cartilage volume.
Collagenases (MMP-1 and MMP-13) cleave collagen, and other metalloproteinases such as stromelysin (MMP-3) and gelatinases (MMP-2 and MMP-9) are also present in the extracellular matrix. MMPs are secreted by chondrocytes in an inactive form. Extracellular activation then leads to the degradation of both collagen and proteoglycans around chondrocytes.
Tissue inhibitors of metalloproteinases (TIMPs) regulate the MMPs. Disturbance of this regulation may lead to an increase in cartilage degradation over synthesis and contribute to the development of OA. TIMPs have not yet proven to be of therapeutic value.
Osteoprotegerin (OPG), RANK and RANK ligand (RANKL) control the remodelling of subchondral bone remodelling. Their levels are significantly different in OA chondrocytes. Inhibiting RANKL may prove a new therapeutic approach in OA.
Aggrecanase production is stimulated by pro-inflammatory cytokines and aggrecan (the major proteoglycan) levels fall.
Synovial inflammation is present in OA, and CRP in the serum may be raised. Interleukin-1 (IL-1) and tumour necrosis factor (TNF-α) release stimulates metalloproteinase production and IL-1 inhibits type II collagen production. IL-6 and IL-8 may also be involved. Anticytokine therapy has not yet been tested in OA. The production of cytokines by macrophages and of MMPs by chondrocytes in OA are dependent on the transcription factor NF-κB. Inhibition of NF-κB may have a therapeutic role in OA.
IL-1 receptor antagonist genes are associated with radiographic severity of knee OA.
Growth factors, including insulin-like growth factor (IGF-1) and transforming growth factor (TGF-β), are involved in collagen synthesis, and their deficiency may play a role in impairing matrix repair. However, increased TGF-β may cause increased subchondral bone density.
Cartilage breakdown products lead to macrophage infiltration and vascular hyperplasia and IL1-β and TNF-α may contribute to further cartilage degradation.
Vascular endothelial growth factor (VEGF) from macrophages is a potent stimulator of angiogenesis and may contribute to inflammation and neovascularization in OA. Innervation can accompany vascularization of the articular cartilage.
Mutations in the gene for type II collagen (COL2A1) have been associated with early polyarticular OA.
A strong hereditary element underlying OA is suggested by twin studies. Further studies may reveal genetic markers for the disease. The influence of genetic factors is estimated at 35–65%.
In the Caucasian population there is an inverse relationship between the risk of developing OA and osteoporosis.
Gender. In women, weight-bearing sports produce a two- to three-fold increase in risk of OA of the hip and knee. In men, there is an association between hip OA and certain occupations: farming and labouring. OA may flare after the female menopause or after stopping hormone replacement therapy.
Periarticular enthesitis has been proposed as a factor in the pathogenesis of nodal generalized OA (NGOA; p. 515) and is the subject of investigation.
The term primary OA is sometimes used when there is no obvious known predisposing factor.
Box 11.4 shows some of the predisposing factors for the development of OA, and Table 11.12 shows other conditions that sometimes cause secondary arthritis.
Table 11.12 Causes of osteoarthritis
Primary OA |
No known cause |
Secondary OA |
Pre-existing joint damage: |
Rheumatoid arthritis |
|
Gout |
|
Spondyloarthritis |
|
Septic arthritis |
|
Paget’s disease |
|
Avascular necrosis, e.g. corticosteroid therapy |
|
Metabolic disease: |
|
Chondrocalcinosis |
|
Hereditary haemochromatosis |
|
Acromegaly |
|
Systemic diseases: |
|
Haemophilia – recurrent haemarthrosis |
|
Haemoglobinopathies, e.g. sickle cell disease |
|
Neuropathies |
Clinical features
Osteoarthritis affects many joints, with diverse clinical patterns. Hip and knee OA are major causes of disability. Early OA is rarely symptomatic unless accompanied by a joint effusion, whilst advanced radiological and pathological OA is not always symptomatic.
Some flare-ups are due to inflammation and there may be a slight rise in ESR or CRP. Focal synovitis is caused by fragments of shed bone or cartilage. Radiological OA is usually, but not inevitably, progressive. This progression may be stepwise or continual. Radiological improvement is uncommon but has been observed, suggesting that repair is possible.
Clinical subsets
Localized OA
Nodal OA (Table 11.13)
Joints of the hand are usually affected one at a time over several years, with the distal interphalangeal joints (DIPs) being more often involved than the proximal interphalangeal joints (PIPs). Nodal OA often starts around the female menopause. The onset may be painful and associated with tenderness, swelling and inflammation and impairment of hand function. At this stage, enthesitis can be seen on MRI. An intra-articular corticosteroid injection can be used at this stage, if deemed necessary. The inflammatory phase settles after some months or years, leaving painless bony swellings posterolaterally: Heberden’s nodes (DIPs) and Bouchard’s nodes (PIPs), along with stiffness and deformity (Fig. 11.12). Functional impairment is slight for most, although PIP osteoarthritis restricts gripping more than DIP involvement. On X-ray, the nodes are marginal osteophytes and there is joint space loss.
Table 11.13 Features of nodal OA

Figure 11.12 Severe nodal osteoarthritis. The DIP joints demonstrate Heberden’s nodes (arrows). The middle finger DIP joint is deformed and unstable. The thumb is adducted and the bony swelling of the first carpometacarpal joint is clearly shown – ‘the squared hand of nodal OA’.
Thumb base OA co-exists with nodal OA and causes pain and disability, which decrease as the joint stiffens. The ‘squared’ hand in OA (Fig. 11.12) is caused by bony swelling of the carpometacarpal joint and fixed adduction of the thumb. Function is rarely severely compromised.
Polyarticular hand OA is associated with a slightly increased frequency of OA at other sites.
Hip OA (see p. 494) affects 7–25% of adult Caucasians but is significantly less common in black African and Asian populations. There are two major subgroups defined by the radiological appearance. The most common is superior-pole hip OA, where joint space narrowing and sclerosis predominantly affect the weight-bearing upper surface of the femoral head and adjacent acetabulum. This is most common in men and unilateral at presentation, although both hips may become involved because the disease is progressive. Early onset of hip OA is associated with acetabular dysplasia or labral tears. Less commonly, medial cartilage loss occurs. This is most common in women and associated with hand involvement (nodal generalized OA – NGOA), and is usually bilateral. It is more rapidly disabling.
The prevalence of symptomatic knee OA is 40% in individuals aged over 75 years. It is commoner in women than in men. There is a strong relationship with obesity. The disease is generally bilateral and strongly associated with nodal OA of the hand in elderly women, or as part of generalized OA. The medial compartment is most commonly affected and leads to a varus (bow-legged) deformity. There is often also retropatellar OA. Previous trauma, meniscal and cruciate ligament tears are risk factors for developing knee OA. Bone marrow lesions seen on MRI predict disease progression and eventual joint replacement.
This is rare but is usually seen in combination with nodal OA – NGOA. The other joints affected are the knees, first MTP, hip, and intervertebral (spondylosis). Its onset is often sudden and severe. There is a female preponderance and a strong familial tendency. Periarticular ligamentous pathology may have an important role in the phenotypic expression of NGOA.
This is rare. The DIPs and PIPs are inflamed and equally affected and the functional outcome is poor. Radiologically, there is marked osteolysis. Destructive phases are followed by phases of remodelling.
This is most commonly seen with calcium pyrophosphate deposition in the cartilage (chondrocalcinosis). Chondrocalcinosis increases in frequency with age and is seen on over 40% of knee X-rays in the over-80s, but is usually asymptomatic. The joints most commonly affected are the knees (hyaline cartilage and fibrocartilage) and wrists (triangular fibrocartilage, see Fig. 11.10). There is patchy linear calcification on X-ray (Fig. 11.13).
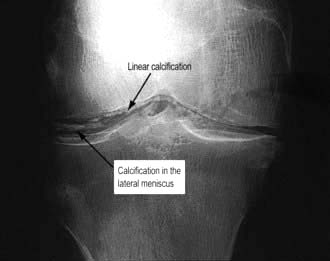
Figure 11.13 Chondrocalcinosis of the knee. Note the linear calcification in the hyaline cartilage and calcification of the lateral meniscus (plus mild secondary OA).
A chronic arthropathy (pseudo-OA) occurs, predominantly in elderly women with severe chondrocalcinosis. There is a florid inflammatory component and marked osteophyte and cyst formation visible on X-rays. The joints affected differ from NGOA, being predominantly the knees, then wrists and shoulders. Chondrocalcinosis is associated with pseudogout, an acute crystal-induced arthritis (see p. 532).
A rare, rapidly destructive arthritis in elderly women, affecting shoulders, hips and knees, is associated with finding crystals of calcium apatite in a bloody joint effusion. The outlook is poor and joints require early surgical replacement.
Investigations in OA
Blood tests. There is no specific test; the ESR is normal although high sensitivity CRP may be slightly raised. Rheumatoid factor and antinuclear antibodies are negative.
X-rays are abnormal only when the damage is advanced. They are useful in preoperative assessments. For knees, a standing X-ray (stressed) is used to assess cartilage loss and ‘skyline’ views in flexion for patello-femoral OA.
MRI demonstrates meniscal tears, early cartilage injury and subchondral bone marrow changes (osteochondral lesions).
Arthroscopy reveals early fissuring and surface erosion of the cartilage.
Aspiration of synovial fluid (if there is a painful effusion) shows a viscous fluid with few leucocytes (p. 498).
Management
The guiding principle is to treat the symptoms and disability, not the radiological appearances; depression and poor quadriceps strength are better predictors of pain than is radiological severity in OA of the knee. Education of the individual about the disease and its effects reduces pain, distress and disability and increases compliance with treatment. Psychological or social factors alter the impact of the disease.
Weight loss and exercises for strength and stability are useful. Hydrotherapy helps, especially in lower-limb OA. Local heat, ice packs, massage and rubefacients or local NSAID gels are all used. Insoles for flat feet and a walking stick held on the contralateral side to the affected lower limb joint are useful.
There is increasing evidence that acupuncture helps knee OA. Other forms of complementary medicine are commonly used and, despite lack of scientific evidence, little is lost in trying it since a number of patients do seem to be helped.
Balance the potential benefit against potential side-effects, especially in the elderly. Paracetamol is effective and should be prescribed before NSAIDs (Box 11.3). NSAIDs or coxibs should be used intermittently when possible. Opioids should be used cautiously in older patients.
Intra-articular corticosteroid injections produce short-term improvement when there is a painful joint effusion. Frequent injections into the same joint should be avoided. The role of intra-articular hyaluronan preparations is unclear.
Glucosamine and chondroitin (sold as food supplements) have no clinically relevant effect on joint pain or joint space narrowing.
There are no proven agents which halt or reverse OA, although they are greatly needed. The role of bisphosphonates in reducing bone changes is unclear. The role of drugs which block tissue metalloproteinases or cytokines (see pathogenesis, below) is also unclear.
Arthroscopy for knee OA is not beneficial. However, replacement arthroplasty has transformed the management of severe OA. The safety of hip and knee replacements is now equal, with a complication rate of about 1%; loosening, and late blood-borne infection are the most serious. The slight but definite risks make it essential that the patient is certain that surgery is necessary. Resurfacing hip surgery has become popular but may have higher complication rates in women. Unicompartmental knee replacement is a less major procedure and appropriate for some patients. For the vast majority, a total hip or knee replacement reduces pain and stiffness, greatly increases function and mobility, and – particularly significant for the elderly – independence.
Other surgical procedures include realignment osteotomy of the knee or hip, excision arthroplasty of the first MTP and base of the thumb, and fusion of a first MTP joint.
Inflammatory arthritis
Inflammatory arthritis (Table 11.14) includes a large number of arthritic conditions in which the predominant feature is synovial inflammation (Box 11.5). This disparate group includes post-viral arthritis, rheumatoid arthritis, spondyloarthritis, crystal arthritis, and Lyme arthritis. The diagnosis of these conditions is helped by the pattern of joint involvement (symmetrical or asymmetrical; large or small) (Table 11.14), along with any non-articular disease; a past and family history is helpful. The periodicity of the arthritis (single acute, relapsing, chronic and progressive) also helps in the diagnosis.
Table 11.14 Pattern of joint involvement in inflammatory arthritis
Diseases presenting as an inflammatory monoarthritis |
Diseases presenting as an inflammatory polyarthritis |
Certain non-articular diseases, e.g. psoriasis, iritis, inflammatory bowel disease, nonspecific urethritis or recent dysentery, suggest spondyloarthritis. There may be evidence of recent viral illness (rubella, hepatitis B or erythrovirus), of rheumatic fever, or a tick bite and skin rash (Lyme disease). In early arthritis, it may not be possible to make a specific diagnosis until the disease has evolved from an undifferentiated arthritis into a chronic form.
There is a distinct genetic separation of rheumatoid-pattern synovitis and spondyloarthritis; RA (see below) is associated with a genetic marker in the class II major histocompatibility genes, whilst spondyloarthritis shares certain alleles in the B locus of class I MHC genes, usually B27 (see p. 526).
In general, the pain and stiffness of inflammatory arthritis are worse in the morning often for several hours, in contrast to the much shorter morning stiffness of OA. Inflammatory markers (ESR and CRP) are often raised in inflammatory arthritis, and there is often a normochromic, normocytic anaemia. Specific types of arthritis are discussed below.
Early inflammatory polyarthritis
Undifferentiated polyarthritis requires urgent referral to a rheumatologist for diagnosis and treatment, including the early introduction of disease-modifying agents when indicated (see p. 523). In persistent inflammatory arthritis sustained remission depends on rapid diagnosis and intensive treatment. Poor prognostic features for undifferentiated polyarthritis are:
Rheumatoid arthritis (ra)
Rheumatoid arthritis is an autoimmune disease associated with autoantibodies to the Fc portion of immunoglobulin G (rheumatoid factor) and to citrullinated cyclic peptide. There is persistent synovitis, causing chronic symmetrical polyarthritis and systemic inflammation. Genetic studies suggest that RA is a heterogeneous group of diseases. Before the modern drug era it was rapidly disabling for most patients.
Epidemiology
RA has a worldwide distribution and affects 0.5–1% (with a female preponderance of 3:1) of the population. The prevalence is low in black Africans and Chinese people. The incidence is falling. RA remains a significant cause of disability and mortality and carries a high socioeconomic cost. It presents from early childhood (when it is rare) to late old age. The most common age of onset is between 30 and 50 years.
Aetiology and pathogenesis
The cause is multifactorial and genetic and environmental factors play a part.
Gender. Women before the menopause are affected three times more often than men. After the menopause, the frequency of onset is similar between the sexes, suggesting an aetiological role for sex hormones. A meta-analysis of the use of the oral contraceptive pill has shown no effect on RA overall, but it may delay the onset of disease.
Familial. The disease is familial with an increased incidence in first-degree relatives and a high concordance amongst monozygotic twins (up to 15%) and dizygotic twins (3.5%). In occasional families it affects several generations.
Genetic factors account for about 60% of disease susceptibility. There is a strong association between susceptibility to RA and certain HLA haplotypes: HLA-DR4, which occurs in 50–75% of patients and correlates with a poor prognosis, as does possession of certain shared alleles of HLA-DRB1*04. The possession of these shared epitope alleles in HLA-DRB1 (S2 and S3P) increases susceptibility to RA and may predispose to anti-citrullinated peptide antibodies (ACPA). Citrullination is a process which modifies antigens, allowing them to fit into the shared epitope on HLA alleles. In a genome-wide association study in ACPA-positive RA, an association was found with loci near HLA-DRBI and PTPN22 in people of European descent. These genes affect the presentation of autoantigens (HLA-DRBI), T cell receptor signal transduction (PTPN22) and targets of ACPA (PAD14).
Smoking is an environmental risk factor for seropositive RA, possibly by activation of the innate immune system.
RA is primarily a synovial disease which invades local tissues and rheumatoid synovitis results when chemoattractants produced in the joint recruit circulating inflammatory cells. Overproduction and overexpression of tumour necrosis factors (TNF) is a key inflammatory element in RA, leading to synovitis and joint destruction. Interaction of macrophages and T and B lymphocytes drives this overproduction. TNF-α stimulates overproduction of interleukin-6 and other cytokines. Antibodies to TNF-α and IL-6 or specific blocking agents produce marked short-term improvement in synovitis, indicating the pivotal role of these cytokines in the chronic synovitis (see p. 523). These antibodies also reduce the malaise and tiredness felt in active RA. Interleukin-1 plays a bigger role in certain subsets, such as systemic juvenile idiopathic arthritis (see p. 545) and adult-onset Still’s disease (see p. 545).
An imbalance in the number of certain cell types appears to be central to immune regulation and its dysfunction.
Synovial cells in chronic rheumatoid synovitis are predominantly abnormally behaving fibroblast-like synoviocytes, and macrophage-like synoviocytes which produce pro-inflammatory cytokines.
Abnormal fibroblast-like synoviocytes appear to circulate between joints and may be the trigger for the polyarthritis.
Osteoclasts play an active role in bone and cartilage destruction.
B cells in the synovium, activated by cytokine-activated macrophages and T cells produce autoantibodies of which IgM and IgA RF is the most typical in RA. As RFs have the Fc portion of IgG as their antigen they have the potential for self aggregation and immune complex formation in the synovium. These may then trigger macrophages via IgGFc receptors to produce even more cytokines including IL-1, IL-8, TNF-α and granulocyte-macrophage colony-stimulating factor, and fibroblasts to produce IL-6.
CD20 positive B cell ablation (a technique used for treating B cell lymphomas) induces temporary remission, reinforcing the central role of B cells in the chronic inflammation of RA. As the B cells return, the CRP rises and the disease flares again.
Synovial fibroblasts have high levels of the adhesion molecule, vascular cell adhesion molecule (VCAM-1: a molecule which supports B lymphocyte survival and differentiation), decay accelerating factor (DAF: a factor that prevents complement-induced cell lysis) and cadherin-II (which mediates cell to cell interactions). These molecules may facilitate the formation of ectopic lymphoid tissue in synovium. Recent studies have shown that mice deficient in cadherin-II are resistant to a form of inflammatory arthritis. High-affinity antibodies are not a feature of RA, unlike other autoimmune diseases.
T cells can be a part of the destructive process but other subsets reduce its severity. T cell-associated cytokines such as IL-2 and IL-4 are not present in high amounts and, when CD4-specific antibodies were used therapeutically to produce a specific helper T cell lymphopenia, they did not significantly alter the disease, suggesting that T cells play a lesser role. This treatment is no longer used. T17 helper cells (see p. 61), which produce IL-17A, 17F, 21 and 22 and TNF-α, may cause inflammation. The normal regulatory T cells are suppressed by TGP-β and interleukins (produced by macrophages and dendritic cells), allowing the T17 helper cells to increase.
The role of innate immunity in RA pathogenesis and in predisposing the joint to inflammation are the subjects of increasing interest (see p. 51).
The triggering antigen, which leads to self-maintained inflammation in RA, remains unclear. Triggers for ACPA production include filaggrin, type II collagen and vimentin. There is little evidence that collagen type II is the triggering antigen, although it is a cause of arthritis in animal models of RA. Smoking is a potential trigger, particularly in ACPA-positive RA.
Pathology
Rheumatoid arthritis is typified by widespread persistent synovitis (inflammation of the synovial lining of joints, tendon sheaths or bursae). The normal synovium is thin and comprises a lining layer a few cells thick containing fibroblast-like synoviocytes and macrophages overlying loose connective tissue. The synoviocytes play a central role in synovial inflammation. In RA the synovium becomes greatly thickened and causes ‘boggy’ swelling around the joints and tendons. There is proliferation of the synovium into folds and fronds, and it is infiltrated by a variety of inflammatory cells, including polymorphs, which transit through the tissue into the joint fluid, and lymphocytes and plasma cells. There are disorganized lymphoid follicles. The normally sparse surface layer of lining cells becomes hyperplastic and thickened (Fig. 11.14). There is marked vascular proliferation. Increased permeability of blood vessels and the synovial lining layer leads to joint effusions that contain lymphocytes and dying polymorphs.
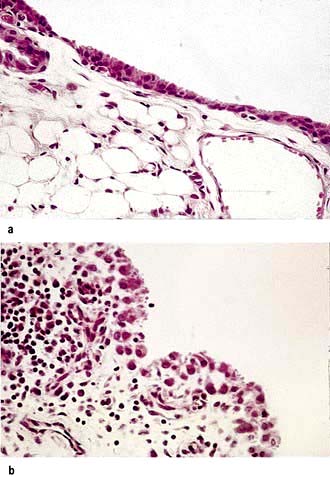
Figure 11.14 Histological appearance of RA synovium. (a) Normal synovium. (b) Synovial appearances in established RA, showing marked hypertrophy of the tissues with infiltration by lymphocytes and plasma cells.
(From Shipley M. Colour Atlas of Rheumatology, 3rd edn. London: Mosby-Wolfe; 1993, with permission.)
The hyperplastic synovium spreads from the joint margins on to the cartilage surface. This ‘pannus’ of inflamed synovium damages the underlying cartilage by blocking its normal route for nutrition and by the direct effects of cytokines on the chondrocytes. The cartilage becomes thinned and the underlying bone exposed. Local cytokine production and joint disuse combine to cause juxta-articular osteoporosis during active synovitis.
Fibroblasts from the proliferating synovium also grow along the course of blood vessels between the synovial margins and the epiphyseal bone cavity and damage the bone. This is shown by MRI to occur in the first 3–6 months following onset of the arthritis, and before the diagnostic, ill-defined juxta-articular bony ‘erosions’ appear on X-ray (Fig. 11.15). This early damage justifies the use of DMARDs (see p. 523) within 3–6 months of onset of the arthritis. Low-dose steroids delay and anti-TNF-α agents halt and occasionally reverse erosion formation. Erosions lead to a variety of deformities and contribute to long-term disability.

Figure 11.15 X-ray of early RA, showing typical erosions at the thumb (black and white arrows) and middle MCP joints (black arrow) and at the ulnar styloid (white arrow).
Rheumatoid factors (RFs) and anti-citrullinated peptide antibodies (ACPAs)
RFs (see p. 496) are circulating autoantibodies that have the Fc portion of IgG as their antigen. Transient production of RF is an essential part of the body’s normal mechanism for removing immune complexes, but in RA they show a much higher affinity and their production is persistent and occurs in the joints. They are of any immunoglobulin class (IgM, IgG or IgA), but the most common tests employed clinically detect IgM rheumatoid factor. Around 70% of people with polyarticular RA have IgM rheumatoid factor in the serum. Positive titres can predate the onset of RA.
The term ‘seronegative RA’ is used for patients in whom the standard tests for IgM rheumatoid factor are persistently negative. They tend to have a more limited pattern of synovitis.
IgM rheumatoid factor is not diagnostic of RA and its absence does not rule the disease out; however, it is a useful predictor of prognosis. A persistently high titre in early disease implies more persistently active synovitis, more joint damage and greater disability eventually, and justifies earlier use of DMARDs.
Anti-CCP antibodies (ACPA) (p. 497) are usually present with RF in RA. They are better predictors of a transition from early transient inflammatory arthritis to persistent synovitis and early RA. RF and the ACPA together are even more specific.
Clinical features of ra
Typical presentation
The most typical presentation of rheumatoid arthritis (approximately 70% of cases) begins as a slowly progressive, symmetrical, peripheral polyarthritis, evolving over a period of a few weeks or months. The patient is usually between 30 and 50 years of age, but the disease can occur at any age. Less commonly (15%) a rapid onset can occur over a few days (or explosively overnight) with a severe symmetrical polyarticular involvement, especially in the elderly. Factors which indicate a poor prognosis are listed in Box 11.6. The differential diagnosis of early RA is shown in Box 11.7.
Older classification criteria used to distinguish RA from other forms of arthritis (American College of Rheumatology, ACR criteria 1987) are now mainly used to ensure matched groups for research. The newer criteria that have replaced them are more suitable for assessing early arthritis because they do not rely on later changes such as erosions and extra-articular disease (Box 11.8).
Box 11.8
ACR/EULAR 2010 criteria for RA
| Criteria | Points |
|---|---|
1. Joint involvement |
0–5 |
1 medium to large joint |
0 |
2–10 medium to large joints |
1 |
1–3 small joints (large joints not counted) |
2 |
4–10 small joints (large joints not counted) |
3 |
>10 joints at least one small joint |
5 |
2. Serology |
0–3 |
Negative RF and negative ACPA |
0 |
Low positive RF or low positive ACPA |
2 |
High positive RF or high positive ACPA |
3 |
3. Acute-phase reactants |
0–1 |
Normal CRP and normal ESR |
0 |
Abnormal CRP or abnormal ESR |
1 |
4. Duration of symptoms |
0–1 |
<6 weeks |
0 |
≥6 weeks |
1 |
The cut-off point for RA is at 6 or more points. Patients can also be classified as having RA if they have both typical erosions and longstanding disease previously satisfying the classification criteria. (Adapted from Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet 2010; 376:1094–1108.)ACR, American College of Rheumatology
In early RA, the combination of at least one swollen joint for more than 6 weeks with no prior injury and no associated history or family history of spondyloarthritis or associated conditions such as psoriasis (see p. 1207) and a positive ACPA test is the best way to select patients for earlier treatment to avoid joint damage. This earlier treatment is evidence based and has been shown to reduce the risk of the development of damage and thus reduce permanent joint deformities.
Symptoms and signs
The majority of patients complain of pain and stiffness of the small joints of the hands (metacarpophalangeal, MCP; proximal and distal interphalangeal, PIP, DIP) and feet (metatarsophalangeal, MTP). The wrists, elbows, shoulders, knees and ankles are also affected. In most cases, many joints are involved, but 10% present with a monoarthritis of the knee or shoulder or with carpal tunnel syndrome.
Fatigue is a common complaint. The pain and stiffness are significantly worse in the morning. Sleep is disturbed.
The joints are usually warm and tender with some joint swelling. There is limitation of movement and muscle wasting. Deformities and non-articular features develop if the disease cannot be controlled (see below).
RA in the older patient may mimic polymyalgia rheumatica; the synovitis becomes apparent as the corticosteroid dose is reduced.
Other presentations
The presentation and progression of RA is variable. Presentations are shown in Box 11.9. Relapses and remissions occur either spontaneously or on drug therapy. In some patients, the disease remains active, producing progressive joint damage. Rarely, the process may cease (‘burnt-out RA’).
Box 11.9
Presentations of rheumatoid arthritis
Palindromic: Palindromic monoarticular attacks lasting 24–48 hours; 50% progress to other types of RA.
Transient: A self-limiting disease, lasting less than 12 months and leaving no permanent joint damage. Usually seronegative for IgM rheumatoid factor and ACPA. Some of these may be undetected post-viral arthritis.
Remitting: There is a period of several years during which the arthritis is active but then remits, leaving minimal damage.
Chronic, persistent: The most typical form, it may be seropositive or seronegative for IgM rheumatoid factor. The disease follows a relapsing and remitting course over many years. Seropositive (plus ACPA) patients tend to develop greater joint damage and long-term disability. They warrant earlier and more aggressive treatment with disease-modifying agents.
Rapidly progressive: The disease progresses remorselessly over a few years and leads rapidly to severe joint damage and disability. It is usually seropositive (plus ACPA), has a high incidence of systemic complications and is difficult to treat.
Seronegative RA initially affects the wrists more often than the fingers and has a less symmetrical joint involvement. It has a better long-term prognosis, but some cases progress to severe disability. This form can be confused with psoriatic arthropathy, which has a similar distribution (p. 528).
Palindromic rheumatism is unusual (5%) and consists of short-lived (24–72 hours) episodes of acute monoarthritis. The joint becomes acutely painful, swollen and red, but resolves completely. Further attacks occur in the same or other joints. About 50% go on to develop typical chronic rheumatoid synovitis after a delay of months or years. The rest remit or continue to have acute episodic arthritis. The detection of RF or ACPA predicts conversion to chronic, destructive synovitis.
Complications (Table 11.15)
This is a serious complication with significant morbidity and mortality. In immunosuppressed patients, the affected joints may not be hot and inflamed with accompanying fever. There is usually a neutrophil leucocytosis. Any effusion, particularly of sudden onset, should be aspirated. Staphylococcus aureus is the most common organism. Blood cultures are often positive. Treatment is with systemic antibiotics (see p. 533) and drainage.
Table 11.15 Complications of rheumatoid arthritis
Side-effects of therapy |
|
|
Amyloidosis (see p. 1042) is found in a very small number of people with uncontrolled rheumatoid arthritis. RA is the most common cause of secondary AA amyloidosis. AL amyloidosis causes a polyarthritis that resembles RA in distribution and is also often associated with carpal tunnel syndrome and subcutaneous nodules.
Joint involvement in RA
The changes described below are seen in established disease or when early drug treatment has been ineffective.
The impact of RA on the hands is severe. In early disease, the fingers are swollen, painful and stiff. Inflamed flexor tendon sheaths increase functional impairment and may cause a carpal tunnel syndrome. Joint damage causes:
A combination of ulnar drift and palmar subluxation of the MCPs (Fig. 11.16). This leads to unsightly deformity, but function may be remarkably good once the patient has learned to adapt, and pain is controlled
Fixed flexion (buttonhole or boutonnière deformity) or fixed hyperextension (swan-neck deformity) of the PIP joints, which impairs hand function
Swelling and dorsal subluxation of the ulnar styloid, which leads to wrist pain and may cause rupture of the finger extensor tendons, leading in turn to a sudden onset of finger drop of the little and ring fingers predominantly, which needs urgent surgical repair.

RA commonly affects the shoulders. Initially, the symptoms mimic rotator cuff tendonosis (see p. 500) with a painful arc syndrome and pain in the upper arms at night. As the joints become more damaged, global stiffening occurs. Late in the disease rotator cuff tears are common (see p. 501) and interfere with dressing, feeding and personal toilet.
Synovitis of the elbows causes swelling and a painful fixed flexion deformity. In late disease, flexion may be lost and severe difficulties with feeding result, especially combined with shoulder, hand and wrist deformities.
One of the earliest manifestations of RA is painful swelling of the MTP joints.
The foot becomes broader and a hammer-toe deformity develops.
Exposure of the metatarsal heads to pressure by the forward migration of the protective fibrofatty pad (Fig. 11.17) causes pain.
Ulcers or calluses may develop under the metatarsal heads and over the dorsum of the toes.
Mid- and hindfoot RA causes a flat medial arch and loss of flexibility of the foot.
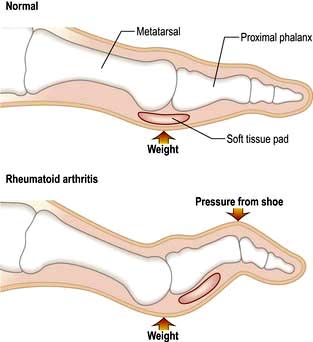
Figure 11.17 The toes in RA, showing exposure of the metatarsal heads with forward migration of the soft tissue pad.
Appropriate broad, deep, cushioned shoes are essential but rarely wholly adequate, and walking is often painful and limited. Podiatry helps and surgery may be required.
Massive synovitis and knee effusions occur, but respond well to aspiration and steroid injection (see p. 507). A persistent effusion increases the risk of popliteal cyst formation and rupture (see p. 508). In later disease, erosion of cartilage and bone causes loss of joint space on X-ray and damage to the medial and/or lateral and/or retropatellar compartments of the knees. Depending on the pattern of involvement, the knees may develop a varus or valgus deformity. Secondary OA follows. Total knee replacement is often the only way to restore mobility and relieve pain.
The hips are occasionally affected in early RA but are less commonly affected than the knees at all stages of the disease. Pain and stiffness are accompanied by radiological loss of joint space and juxta-articular osteoporosis. The latter may permit medial migration of the acetabulum (protrusio acetabulae). Later, secondary OA develops. Hip replacement is usually necessary.
Painful stiffness of the neck in RA is often muscular, but it may be due to rheumatoid synovitis affecting the synovial joints of the upper cervical spine and the bursae which separate the odontoid peg from the anterior arch of the atlas and from its retaining ligaments. This synovitis leads to bone destruction, damages the ligaments and causes atlantoaxial or upper cervical vertebral instability. Subluxation and local synovial swelling may damage the spinal cord, producing pyramidal and sensory signs. MRI is the best way of visualizing this, but lateral flexed and extended neck X-rays can demonstrate instability. In late RA, difficulty walking which cannot be explained by articular disease, weakness of the legs or loss of control of bowel or bladder may be due to spinal cord compression and is a neurosurgical emergency.
Image the cervical spine in flexion and extension in people with RA before surgery or upper gastrointestinal endoscopy to check for instability and reduce the risk of cord injury during intubation.
Non-articular manifestations (Fig. 11.18)
Soft tissue surrounding joints
Subcutaneous nodules are firm, intradermal and generally occur over pressure points, typically the elbows, the finger joints and the Achilles tendon. Histologically, there is a necrotic centre surrounded by rows of activated macrophages, which resembles synovitis without a synovial space.
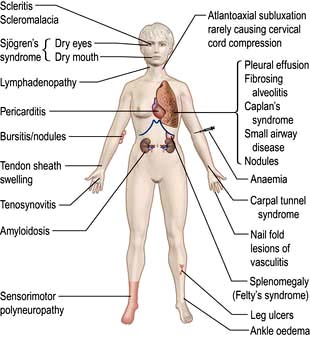
The nodules may ulcerate and become infected. They may resolve when the disease comes under control. The nodules can be removed surgically but they tend to recur.
The olecranon and other bursae may be swollen (bursitis).
Tenosynovitis of flexor tendons in the hand can cause stiffness and occasionally a trigger finger. Swelling of the extensor tendon sheath over the dorsum of the wrist is common.
Muscle wasting around joints is common. Corticosteroid-induced myopathy occurs. Osteoporosis is more common in poorly controlled RA.
Less common non-articular manifestations
Non-articular complications are becoming less common, probably because of more effective disease control.
Lungs (see p. 792)
Airways disease: a spectrum from predominant bronchiectasis (cough and daily sputum) to predominant obliterative bronchiolitis (progressive breathlessness)
Disease of the pleura: pleural effusion (asymptomatic to mildly breathless) and thickening
Fibrosing alveolitis: a combination of inflammation and basal lung fibrosis
Peripheral, intrapulmonary nodules: these are asymptomatic but may cavitate, especially with pneumoconiosis (Caplan’s syndrome)
Infective lesions, e.g. TB in patients on biological DMARDs.
Vasculitis (see p. 542) is caused by immune complex deposition in arterial walls. It is uncommon. Smoking is a risk factor. Findings are:
Nail-fold infarcts due to cutaneous vasculitis
Widespread cutaneous vasculitis with necrosis of the skin (seen in people with very active, strongly seropositive disease)
Mononeuritis multiplex (p. 1145)
Necrotizing arteritis of the mesenteric vessels causing bowel infarction.
The heart and peripheral vessels
Poorly controlled RA with a persistently raised CRP and high cholesterol is a risk factor for premature coronary artery and cerebrovascular atherosclerosis independent of traditional risk factors (i.e. high cholesterol and hypertension). Other cardiovascular problems include:
Pericarditis is rarely symptomatic.
Endocarditis and myocardial disease, rarely symptomatic, are found at post-mortem in approximately 20% of cases.
Raynaud’s syndrome occurs (see p. 788).
Sicca syndrome causes dry mouth and eyes (see Sjögren’s syndrome, p. 541).
Scleritis and episcleritis occur in severe, seropositive disease, resulting in painful red eye.
Amyloidosis causes proteinuria, nephrotic syndrome and chronic kidney disease. It occurs rarely in severe, longstanding rheumatoid disease and is due to the deposition of highly stable serum amyloid A protein (SAP) in the intercellular matrix of a variety of organs. SAP is an acute-phase reactant, produced normally in the liver.
The spleen, lymph nodes and blood
Felty’s syndrome is splenomegaly and neutropenia in a patient with RA. Leg ulcers or sepsis are complications. HLA-DR4 is found in 95% of patients, compared with 50–75% of people with RA alone.
The lymph nodes may be palpable, usually proximal to affected joints. There may be peripheral lymphoedema of the arm or leg.
Anaemia is almost universal and is usually normochromic and normocytic. It may be iron-deficient owing to gastrointestinal blood loss from NSAID ingestion, or rarely haemolytic (Coombs positive). There may be a pancytopenia due to hypersplenism in Felty’s syndrome or as a complication of DMARD treatment. A high platelet count occurs with active disease.
Diagnosis and investigations
The diagnosis relies on the clinical features described above. The predictors of poor prognosis arthritis are listed in Box 11.6. Initial investigations include:
Blood count. Normochromic, normocytic anaemia may be present.
The ESR and/or CRP are raised in proportion to the activity of the inflammatory process and are useful in monitoring treatment.
Serology. ACPA (see p. 497) is present earlier in the disease (and may predate it by many years), and in early inflammatory arthritis indicates the likelihood of progressing to RA. Rheumatoid factor is present in approximately 70% of cases and ANA at low titre in 30%.
X-rays show soft tissue swelling in early disease but MRI demonstrates synovitis and early erosions.
Aspiration of the joint if an effusion is present. The aspirate looks cloudy owing to white cells. In a suddenly painful joint septic arthritis should be suspected (see p. 532).
Doppler ultrasound is a very effective way of demonstrating persistent synovitis when deciding on the need for DMARDs or assessing their efficacy.
Other investigations will depend on the clinical picture as outlined above. In severe disease, extensive imaging of joints may be required. MRI is the technique of choice, especially for the knee and cervical spine.
Management of ra (box 11.10)
The diagnosis of RA inevitably causes concern and fear in the patient and requires a lot of explanation and reassurance. Most guidelines suggest that anyone with early inflammatory arthritis should be referred to a specialist arthritis clinic within 3 months of onset, whenever possible.
Box 11.10
Management of rheumatoid arthritis
Establish the diagnosis clinically.
Use NSAIDs and analgesics to control symptoms.
Try to induce remission with i.m. depot methylprednisolone 80–120 mg if synovitis persists beyond 6 weeks.
If synovitis recurs, refer to a rheumatologist to start DMARDs and consider combinations of sulfasalazine, methotrexate and hydroxychloroquine. Give a second dose of i.m. depot methylprednisolone or oral steroids.
Refer for physiotherapy and general advice through a specialist team.
As improvement occurs, as measured by less pain, less morning stiffness and reduced acute-phase response, tail-off steroids and possibly reduce drugs.
The doctor should have a positive approach and remind the patient that with the help of drugs most people continue to lead a more or less normal life, despite their arthritis; 25% will recover completely. The earliest years are often the most difficult and people should be helped and encouraged to stay at work during this phase if possible. Uncertainty about remissions and flares and the impact of drug treatment makes planning difficult. However, patients adjust remarkably with time and support; the specialist team in a rheumatology unit (including doctors, nurses, physiotherapists, podiatrists and psychologists) helps patients learn to cope. Leaflets, websites and local patient groups also provide helpful advice.
Patients from socially deprived backgrounds and smokers have a worse prognosis. Statins have been shown to be of benefit in reducing cardiovascular risk and possibly inflammation whatever the cholesterol level; more studies are required.
Drug therapy
There is no curative agent available for RA but drugs are now available that prevent disease deterioration. Symptoms are controlled with analgesia and NSAIDs. Data now support the use of DMARDs early in the disease to prevent the long-term irreversible damaging effects of inflammation of the joints, and drugs that block TNF-α and IL-1 and the use of B cell ablation with rituximab are revolutionizing the management of RA. Searching for persistent synovitis in patients in apparent remission using Doppler ultrasound is leading to more intensive therapeutic regimes which will potentially reduce longer-term disability.
Non-steroidal anti-inflammatory drugs (NSAIDs) and coxibs
Most people with RA are unable to cope without an NSAID to relieve night pain and morning stiffness. NSAIDs do not reduce the underlying inflammatory process. They all act on the cyclo-oxygenase (COX) pathway (see Fig. 15.30). The individual response to NSAIDs varies greatly. It is desirable therefore to try several different drugs for a particular patient in order to find the best (Box 11.13). Each compound should be given for at least a week. Start with an inexpensive NSAID with few side-effects and with which you are familiar. Regular doses are needed to be effective. The major side-effects of NSAIDs and the use of coxibs are discussed on page 511. If gastrointestinal side-effects are prominent, or the patient is over 65 years of age, add a proton pump inhibitor. Slow-release preparations (e.g. slow-release diclofenac, 75 mg, taken after supper), or a suppository at bedtime, usually work well. For additional relief, a simple analgesic is taken as required (e.g. paracetamol or a combination of codeine or dihydrocodeine and paracetamol). Many patients need night sedation.
Corticosteroids
There is evidence to suggest that the early use of corticosteroids slows down the course of the disease but intensive short courses in very early arthritis do not appear to stop progressive disease. Corticosteroids are the commonest cause of secondary osteoporosis. Treatment for more than 3 months or with repeated courses is a risk, and concomitant calcium with vitamin D and bisphosphonates is necessary.
Intra-articular injections with semicrystalline steroid preparations have a powerful but sometimes only short-lived effect.
Intramuscular depot injections (40–120 mg depot methylprednisolone) help whilst waiting for DMARDs to work and to control severe disease flares, or they can be used before a holiday or other life event. They should be used infrequently.
Oral corticosteroids have a number of problems (Boxes 11.11 and 19.11). They are powerful disease-controlling drugs, but are avoided in the long term because side-effects are inevitable. Early intensive short-term regimens are often used. Doses of 5–7.5 mg daily as maintenance therapy are used in some centres. Corticosteroids are invaluable to people with severe disease with extra-articular manifestations such as vasculitis.
Box 11.11
Problems associated with the use of corticosteroids
Patients are increasingly anxious about the use of corticosteroids because of adverse publicity about their potential side-effects. This must be discussed frankly and the risks of not using corticosteroids in treatment should be described and balanced against the risks of the drugs themselves.
Patients must be warned to avoid sugars and saturated fats and to eat less because of the risk of weight gain.
The skin becomes thin and easily damaged.
Monitor for diabetes and hypertension.
Cataract formation may be accelerated.
Osteoporosis develops within 6 months on doses above 7.5 mg daily. Monitor with DXA scan and treat with calcium and vitamin D and bisphosphonate (see this chapter).
Disease-modifying anti-rheumatic drugs (DMARDs)
DMARDs, prescribed by a rheumatologist, are listed in Table 11.16 (see also Fig. 11.19).
Traditional DMARDs, which mainly act through cytokine inhibition, reduce inflammation, with a reduction of joint swelling, a fall in the plasma acute-phase reactants and slowing of the development of joint erosions and irreversible damage. Their beneficial effect is not immediate (hence ‘slow-acting agents’) and may be partial or transient.
DMARDs often only have a partial effect, achieving between 20% and 50% improvement by ACR criteria for disease remission (Box 11.12).
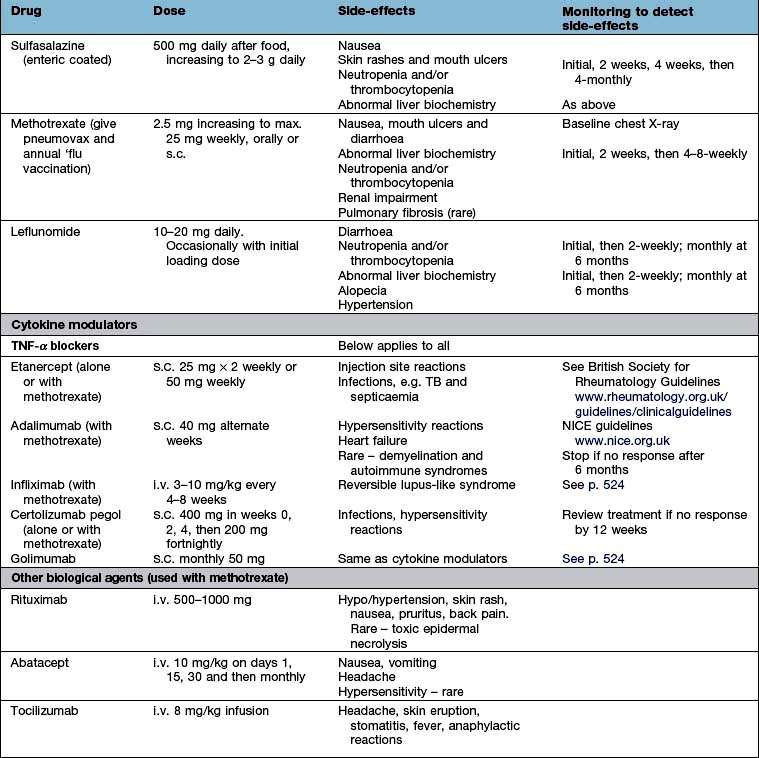
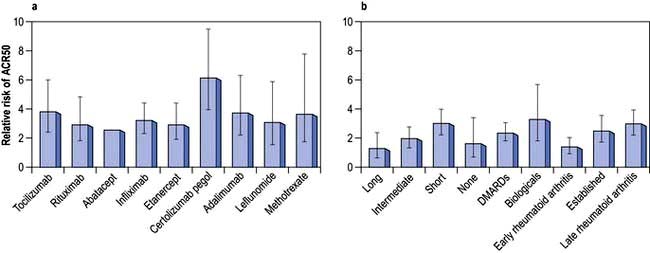
Figure 11.19 American College of Radiology ACR50 responses in trials of DMARDs and biological agents (50% improvement in five of seven measures in the ACR 1987 criteria).a,b (a) ACR50 response in trials of DMARDs and biological agents. (b) Impact of treatment duration, disease stage and prior treatment on ARC50 response. The difference between patients treated with active drug and placebo is greatest in people with late rheumatoid arthritis who have failed biological treatment and whose disease is managed for short periods. The difference is smallest in individuals with early arthritis who have not previously received DMARDs and are treated for a long time. American College of Rheumatology 1987 criteria for diagnosis of RA (revised 1988) have been superseded (see Box 11.8) but are used in trials, with ≥4 criteria necessary for diagnosis: morning stiffness >1 hours for ≥6 weeks; arthritis of ≥3 joints for ≥6 weeks; arthritis of hand joints and wrists for ≥6 weeks; symmetrical arthritis, subcutaneous nodules; positive serum rheumatoid factor; typical radiological changes (erosions and/or periarticular osteopenia). Error bars 95% CIs.
(From Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet 2010; 376:1094–1108, with permission.)
DMARDs are used as early as possible once RA has been diagnosed. Studies suggest that early intervention with DMARDs at 6 weeks to 6 months improves the outcome. Combinations of three or four drugs (steroids, sulfasalazine, methotrexate and hydroxychloroquine) in early RA are increasingly common, reducing the number of agents once remission has been achieved. Most DMARDs are contraindicated in pregnancy (Box 11.13). Effective treatment with DMARDs reduces the increased cardiovascular risk seen in people with RA.
Box 11.13 Drug use during pregnancy in treatment of rheumatoid arthritis
paracetamol – the oral analgesic of choice
Oral NSAIDs and selective COX-2 inhibitors: can be used after implantation up until the last trimester if symptoms justify their use.
Corticosteroids: may be used to control disease flares (main maternal risks are hypertension, glucose intolerance and osteoporosis).
Cytokine modulators: safety during pregnancy is currently unclear.
Contraindicated in breast-feeding: methotrexate, leflunomide, cyclophosphamide, ciclosporin, azathioprine, sulfasalazine, hydroxychloroquine.
This is a combination of sulfapyridine and 5-amino-salicylic acid. Sulfapyridine is probably the active component. It is well tolerated and can be used during pregnancy. Around 50% of patients respond in the first 3–6 months, but efficacy can be lost. Blood monitoring is obligatory because of the risk of leucopenia and thrombocytopenia.
This is considered by many to be the ‘gold standard’ drug in RA. It should not be used in pregnancy. Conception should be delayed for 3–6 months off the drug for either partner. A chest X-ray is taken to exclude tuberculosis. An initial pneumococcal and annual influenza vaccination are given. The starting weekly dose of 2.5–7.5 mg orally is increased up to 15–25 mg if necessary. It is well tolerated and this therapy can be introduced early in the disease. Nausea or poor absorption may limit its efficacy, in which case it is given by subcutaneous injection. Oral folic acid reduces side-effects but may also reduce efficacy. Full blood counts and liver biochemistry should be monitored. It usually works within 1–2 months. More patients remain on this agent than on most other DMARDs, indicating that it is effective and has relatively few side-effects.
A dose of 200–400 g daily is well tolerated. It is used alone in mild disease or as an adjunct to other DMARDs. Retinopathy is extremely rare (occurring in about 1 in 2000 patients on this drug). Some rheumatologists arrange an initial check of macular function with an Amsler chart and further reviews annually, as retinopathy is irreversible.
This DMARD exerts an immunomodulatory effect by preventing pyrimidine production in proliferating lymphocytes through blockade of the enzyme dihydroorotate dehydrogenase, thus blocking clonal expansion of T cells. Most other cells are able to bypass this blockade. It has a long half-life of 4–28 days. A dose of 20 mg daily (10 mg if diarrhoea is a problem) is used. Diarrhoea diminishes with time. Blood monitoring is obligatory (full blood count, platelets, liver biochemistry). The onset of action is 4 weeks with some further improvement sustained at 2 years. Leflunomide works in some patients who have failed to respond to methotrexate. Its long half-life means that it is best avoided in women planning a family.
TNF-α blockers. The availability of agents that block TNF-α has significantly changed the traditional use of DMARDs. Because of their cost they are used after at least two DMARDs (usually sulfasalazine and methotrexate) have been tried. They represent a major therapeutic advance, although not all patients respond and there is loss of efficacy in some responders. They are usually given in combination with methotrexate to reduce loss of efficacy due to antibody formation.
Etanercept is a fully humanized p75 TNF-α receptor IgG1 fusion protein given by self-administered subcutaneous injection. Around 65% of patients respond well. Some develop an injection reaction.
Adalimumab is a fully human monoclonal antibody against TNF-α, given along with methotrexate.
Infliximab is a monoclonal antibody against TNF-α, given intravenously and co-prescribed with methotrexate to prevent loss of efficacy because of antibody formation.
Certolizumab pegol is an Fab fragment of a humanized TNF-α inhibitor monoclonal antibody approved in the UK and other countries. It is PEGylated, i.e. polyethylene glycol groups are added to reduce its immunogenicity and prolong its half-life. The lack of an Fc portion on the antibody aims to reduce the risk of complement-dependent and antibody dependent cytotoxicity. It is useful with or without methotrexate for severe active RA.
Golimumab is a human IgG1-κ monoclonal antibody against TNF which is awaiting approval in some countries. It is given by subcutaneous injection once monthly for severe RA.
These products slow or halt erosion formation in up to 70% of people with RA and produce healing in a few. Malaise and tiredness improve in a manner that is not seen with other DMARDs. Secondary failure occurs with all in the first year and changing to another anti-TNF agent is justified and often regains control of the disease. Potential biomarkers for responsiveness are being studied. Failure to respond to one does not predict failure to others.
Side-effects. Many patients on cytokine modulators are entered into a long-term observational study in the UK and other countries to monitor for potential side-effects. To date, the results are reassuring. People with severe RA are at slightly increased risk of lymphoma and this is being carefully monitored. There is no convincing evidence of any increased risk of other cancers. A few people become ANA positive and develop a reversible lupus-like syndrome, leucocytoclastic vasculitis, some extracutaneous involvement or interstitial lung disease. Reactivation of old TB may occur but is probably less common with etanercept. A pre-treatment chest X-ray is recommended, with a specialist review for high-risk groups. TB should be treated before using these agents and a course of prophylaxis is used in latent disease. There is an increased risk of chest infections which requires close monitoring. Hepatitis B and C infection requires careful risk analysis and regular aminotransferase monitoring if anti-TNF agents are prescribed. They should not be used in patients who have severe cardiac failure.
These agents are extremely expensive when compared with traditional DMARDs but they may save costs in the longer term by reducing disability and the need for hospitalization. Their use should be restricted to specialist centres. To date there is no evidence of an adverse effect on pregnancy outcome but care is essential.
Rituximab is a genetically engineered chimeric monoclonal antibody (p. 72) that causes lysis of CD20-positive B cells. CD20 is a pan-B cell surface antigenic phosphoprotein. Its expression is restricted to pre-B and mature B cells but it is not present on stem cells and is lost before differentiation into plasma cells. Rituximab produces significant improvement in RF-factor positive RA for 8 months to several years when used alone or in combination with corticosteroids and/or methotrexate. This is associated with a 6–9-month B cell lymphopenia with little change in circulating immunoglobulins. A re-flare is often accompanied by a return of peripheral lymphocytes and a rise in CRP. Rituximab can be reused as the disease flares. Repeated courses over up to 5 years are acceptable and well tolerated and around 80% of RF-positive patients respond with 50–60% showing persistent disease control. It is worth trying in patients who have failed to respond to anti-TNF agents. There may be an increased risk of chest infections, and immunoglobulin levels may fall progressively and need to be monitored.
Abatacept is a recombinant fusion protein of CTLA4 and the Fc portion of IgG1, which selectively modulates T cell activation by costimulation blockade. It may have an important role in patients who do not respond to anti-TNF regimens.
Tocilizumab is a humanized monoclonal anti-IL-6 receptor antibody and is used with methotrexate for moderate to severe RA after at least one other cytokine modulator has failed.
Anakinra is a human recombinant IL-1 receptor antagonist which is used in combination with methotrexate. It has been used after anti-TNF agents have been unsuccessful, but is now only recommended for clinical studies.
Spleen tyrosine kinase (SYK) inhibitor given orally has been effective in RA in phase 2 studies.
Drugs used less commonly
Gold (sodium aurothiomalate) is given by deep intramuscular injection. A response (occasionally remission) is seen in about 3 months. Side-effects or lack of effect mean that few patients remain on it beyond 2 years. Blood and urine testing are mandatory.
D-Penicillamine is given before food for at least 3 months before improvement occurs. If proteinuria exceeds 2 g/24 hours the drug must be stopped. Loss of taste is reversible. Other rare side-effects include a lupus erythematosus-like syndrome and a myasthenia gravis-like syndrome.
Azathioprine at a maximum dose of 2.5 mg/kg and cyclophosphamide 1–2 mg/kg have been used, usually when other DMARDs have been ineffective. They are often used when extra-articular features are severe, particularly with vasculitis. There is a high risk of neutropenia and possibly liver toxicity from azathioprine in patients who have low levels of the enzyme thiopurine methyltransferase (TPMT) which metabolizes azathioprine into its active metabolites. Pretesting is a wise precaution.
Ciclosporin 2.5–4 mg/kg is used for active rheumatoid arthritis when conventional therapy has been ineffective. Side-effects include a rise in creatinine level and hypertension.
Physical measures
People with RA need constant advice and support from physiotherapists and nurse specialists, especially while they are learning to adjust. A combination of rest for active arthritis and exercises to maintain joint range and muscle power is essential. Exercise in a hydrotherapy pool is popular and effective. Advice about managing activities of daily living despite the arthritis, and about gadgets, seating or structural changes in the home or at work are helpful. Family and friends should be involved. Podiatry, shoe wear advice and psychological support should be offered to all people with RA.
Surgery
Surgery has a useful role in the long-term approach to patient management but is less frequently needed as therapeutic disease control becomes more effective. Its main objectives are prophylactic, to prevent joint destruction and deformity, and reconstructive, to restore function.
Single-joint disease can be treated by surgical synovectomy to reduce the bulk of inflamed tissue and prevent damage. Excision arthroplasty of the ulnar styloid reduces pain and the risk of extensor tendon damage. Excision arthroplasties of the metatarsal heads reduce metatarsal pain and relieve pressure points. The major surgical advance has been the development of total replacement arthroplasty of the hip, knee, finger joints, elbow and shoulder. Such procedures need careful planning and preparation, and the expected outcomes and risks should be explained to the patient.
Prognosis
A poor prognosis is indicated by:
A clinical picture of an insidious rather than an explosive onset of RA, female sex, increasing number of peripheral joints involved and the level of disability at the onset
Blood tests showing a high CRP/ESR, normochromic normocytic anaemia and high titres of ACPA antibodies and of rheumatoid factor
X-rays with early erosive damage (note: ultrasound and MRI can show cartilage and bone damage prior to conventional X-rays).
Prognosis can be altered dramatically with early DMARD therapy under expert supervision.