16 COMMUNICATING WITH THE DENTAL LABORATORY
To make a high-quality fixed prosthesis, all members of the dental team must understand what they can reasonably expect from each other. A mutual knowledge of individual limitations is crucial. The dentist who does not understand and appreciate the challenges faced by the technician is at a serious disadvantage when prescribing and delegating laboratory procedures (Fig. 16-1). Crucial to the development of sound clinical judgment is a thorough understanding of technical procedures and their rationale, which are described in the chapters of this section.
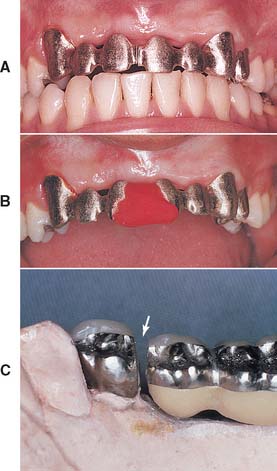
Fig. 16-1 A, This six-unit anterior metal-ceramic framework did not seat. After sectioning between the incisors, the adaptation of the individual components was satisfactory. Note the (correct) narrow width of the soldering gap. B, The two segments indexed with autopolymerizing resin for subsequent soldering. C, The dentist sectioned this fixed dental prosthesis (FDP) incorrectly: the soldering gap is much too wide (arrow), and distortion during soldering will almost certainly result.
DENTAL TECHNOLOGY TRAINING AND CERTIFICATION
The National Association of Dental Laboratories (NADL) is committed to upholding and advancing the commercial dental laboratory industry. This organization emphasizes the following information1:
In 46 states, there are no laws to set minimum qualifications for performance of dental technology or the operation of a dental laboratory. However, several states are moving forward with legislative proposals on “mandated technician certification.” The American Dental Association (ADA) Council on Dental Practice voted in 2005 at the NADL’s request to remove some policy language that was an obstacle to laboratory regulation/technician licensure through certification at the state level.2 Technicians and laboratories that become certified do so as evidence of their commitment to maintaining professional standards in dental technology. There are approximately 52,000 individual dental laboratory technicians in the United States. Because technicians are not required to be registered or licensed in most states, tracking has to come from various government and private sources.
In 2002, 25 programs in dental laboratory technology were approved (accredited) by the Commission on Dental Accreditation in conjunction with the ADA.
The National Board for Certification, an independent board established by the NADL, offers voluntary certification in dental laboratory technology. Certification can be obtained in five specialty areas: crowns and bridges, ceramics, partial dentures, complete dentures, and orthodontic appliances. Certification is required in the states of Kentucky, Texas, and South Carolina. The standards and requirements for certification do not vary across state lines. A certified dental technician (CDT) tested in New England must demonstrate the same competencies as a CDT tested on the Pacific coast.
To qualify for certification, technicians must have a 2-year dental technology degree or at least 5 years’ experience in dental technology and must pass written and practical examinations. To maintain certification, they must document at least 12 hours of continuing education annually, including study of infection control (specific procedures designed to control the spread of disease agents). The requirements for a certified dental laboratory include having a Certified Dental Technician (CDT) present to supervise each department in the specialty, in which they and the laboratory are certified, to ensure that proper safety and production practices are followed. Certification must be renewed annually.*
Technicians who maintain their certification must take 12 hours of continuing education each year, including a required hour in OSHA compliant infection control procedures.
The first CDTs were tested in 1958. Today the National Board for Certification tests more than 1200 technicians annually. In 1978, the current standards for laboratory certification were adopted; today there are more than 400 certified dental laboratories.2
In 2004, the U.S. dental laboratory industry produced approximately $5 billion in sales. The number of dental laboratories in the United States is about 12,000.
MUTUAL RESPONSIBILITIES
Good communication is the key to the technical success of the dental team3-5 This requires a close working relationship between the dentist and laboratory technician. Anticipating satisfactory results is unrealistic if the dentist does not have a reasonable amount of experience with, and a thorough understanding of, dental laboratory procedures. Active participation in the technical procedures by the dentist is paramount, and clinicians who take the time to develop an in-depth understanding of laboratory work make better clinical decisions because of their understanding of applicable technical and material science limitations. Only then can a dentist select the best compromise between technical restrictions, on the one hand, and biologic factors and esthetic needs, on the other. Similarly, if the technician does not appreciate and respect the clinical demands or the treatment rationale of the dentist, the results will be less than satisfactory (Fig. 16-2). The dentist can earn this respect by being prepared to meet personal responsibilities, by listening carefully to technical advice rendered, and by actively participating in the technical decision-making process.

Fig. 16-2 It is often difficult for the technician to appreciate soft tissue contours and embrasure form. These substructures were not fabricated properly—the metal porcelain junction was placed too far facially (arrows). Unless corrected during clinical evaluation, metal would be visible and detract from the appearance of the prosthesis.
Surveys6-8 of fixed prosthodontic laboratories reveal that dentists delegate a significant proportion of their responsibilities. The technicians surveyed were often dissatisfied with the quality of work received; complaints included insufficient information being included in the work authorization, the submission of deficient impressions, and inadequate occlusal records. Such surveys highlight significant problems in dentist-technician communication. In other studies and opinions concerning dentist-technician interaction, whether written by dentists or technicians, the authors emphasized that better patient care is achievable only by better patient care communication.9
The ADA has issued guidelines to improve the relationship between dentist and technicians.10 They are reprinted here:
The Dentist
The Laboratory Technician
RESPONSIBILITIES OF THE DENTIST
The dentist has the overall responsibility for the treatment rendered. Delegating many procedures to auxiliary personnel is possible if all the necessary information is provided to enable them to deliver high-quality service. However, errors such as insufficient tooth reduction, uncertainty about the location of tooth preparation margins, improper interocclusal records and articulations, and ambiguity in communicating the desired shades for esthetic restorations to the technician hamper this responsibility.
Infection Control
The U.S. Department of Health and Human Services11 and the ADA12 have issued guidelines about the disinfection and handling of impressions and other material transferred from the dental office to the dental laboratory. Applicable guidelines are detailed in Chapter 14. Strict adherence to infection control guidelines cannot be overemphasized, because the potential for infection of dental laboratory personnel exists. In a 1990 sample,13 of all materials sent from dental offices to dental laboratories, 67% were contaminated. Results from a more recent questionnaire submitted to dental laboratories suggest that technicians believed in less than 60% of the cases that materials had been appropriately disinfected before being submitted to the laboratory.8
Tooth Preparation
An organized approach to tooth preparation has been discussed in Chapter 7, Chapter 8, Chapter 9, Chapter 10, Chapter 11, which provide the criteria for minimally necessary clearances for the various restorations.
Inadequate tooth reduction in the cervical third for a metal-ceramic restoration is a common error. Obviously, on long clinical crowns of vital teeth (e.g., after periodontal surgery), it is not always possible to reduce the desired 1.2 to 1.5 mm without pulp exposure. Nevertheless, it is generally impossible, even for an experienced ceramist, to achieve superior esthetic results if the tooth is underprepared.14 Inexperienced technicians tend to resolve the problem by overcontouring (Fig. 16-3), but this usually leads to the initiation or recurrence of periodontal disease. Esthetic difficulties and treatment limitations such as these should be discussed with the patient during the treatment planning phase. Communication regarding any deviation from “ideal” criteria ahead of time is essential and can prevent misunderstanding, frustration, and ultimate failure.
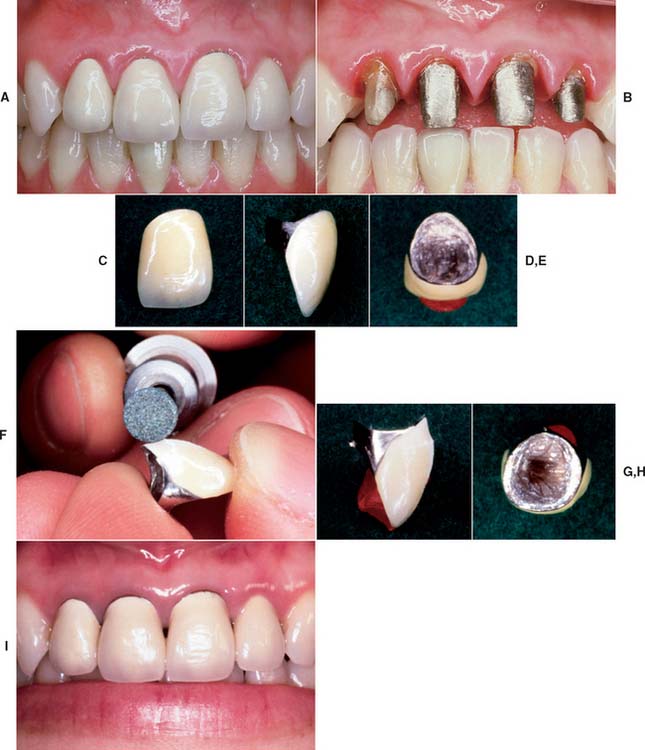
Fig. 16-3 Unrealistic expectations. Restoration failure resulting from excessive axial contours. A, Recently placed metal-ceramic crowns have contributed to gingival inflammation. B, Insufficient shoulder width is seen when the crowns are removed. C and D, Excessive contours: Note the cervical bulge on the facial aspect of this restoration (D). E, A significant amount of axial wall is visible from a gingival view. F to H, The restorations are recontoured and polished. Compare the view in G with that in D and the view in H with that of E. I, Tissue health quickly improves when the recontoured restorations are temporarily recemented. After correction of the underreduced tooth preparations, replacement crowns were made for esthetic reasons.
Preparation Margins
Margins should be easily discernible and accessible on the casts submitted to the technician. The saying “If you can’t see it, you can’t wax it” describes the situation well. (The requirements for dies are listed in Chapter 17.)
The dentist should outline the margins on the dies15 (Fig. 16-4). However, in practice, few dentists do this.16 If the teeth are properly prepared and the impression is accurate, the margins should be obvious, which makes this step unnecessary. When doubt exists, the dentist’s knowledge of the extent of the preparation should resolve any uncertainty.

Fig. 16-4 Marking the preparation margin with a colored pencil. The line must be clearly visible but of minimal thickness.
Dentists must understand the importance of margin design and geometry. For instance, it is unrealistic to request a collarless restoration on a shoulder-bevel type of margin or an all-ceramic crown restoration on a tooth with a narrow chamfer finish line (Figs. 16-5 and 16-6).

Fig. 16-5 The expectations of the dentist are not realistic. These preparations are unsuitable for the metal-ceramic restorations requested, because the gingival one-third was inadequately reduced.

Fig. 16-6 Three types of esthetic restorations. The restoration with the metal collar can be fabricated on a shoulder or shoulder-bevel margin; the porcelain labial margin metal-ceramic crown can be fabricated on a shoulder margin; and the all-ceramic crown requires a slightly rounded internal angle. The latter two require margins that are glasslike in smoothness.
Although an experienced technician will probably bring any unrealistic demands to the attention of the dentist, some well-meaning technicians may attempt to meet a request that is doomed to failure from the beginning. To quote one excellent dentist, “When you discover an error has occurred—STOP! Don’t proceed. Return to the step where the error occurred and correct it. Attempting to blunder on without correcting it properly will only compound and complicate the error.”
Articulation
Proper articulation of opposing casts is the responsibility of the dentist. Often it is advisable to schedule a separate appointment with the patient for verification of the articulation. This is particularly crucial as the complexity of treatment increases (Fig. 16-7). An apparently slight discrepancy may require a remake or hours of corrective grinding and a compromised result. With careful planning, verification of the articulation can be done efficiently and results in peace of mind. Appropriate trimming of interocclusal records should be done by the dentist. Only after trimming is it possible to verify the positional stability of the record on the cast (Fig. 16-8).

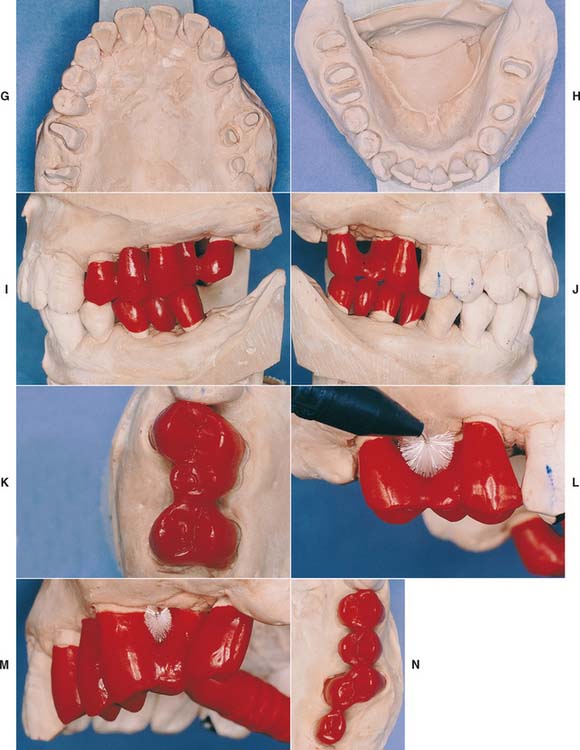



Fig. 16-7 A to F, In the presence of compromised periodontal support, optimal loading is crucial to enhance the prognosis. Accurate occlusion is essential to successful restoration of this periodontally compromised patient for whom multiple hemisections, root resections, and amputations have been performed. Extensive communication with the technician is necessary. G to N, After verification of the articulation, the restorations are waxed to anatomic contour. Wax patterns are designed to combine occlusal function with maximum access for oral hygiene. Note the buccolingual reduction in width of the occlusal table (I) and the emergence profile on the maxillary molars (I and J). O to R, In the bisque stage, the restorations are evaluated, and form is modified as required before indexing and post-soldering. S to X, Glazed and polished restorations on the definitive cast. Note that occlusal rests have already been incorporated in the fixed prostheses in the mandibular arch (T, U, and V) to anticipate possible failure (see Chapter 32). Y to CC, Completed restorations in place. DD to FF, Note that embrasure design allows proper cleaning.

Work Authorization
In some jurisdictions, the written instructions may be referred to as a work authorization, whereas elsewhere it may be referred to as a laboratory work order or prescription. In addition to certain general information that is required by law, a work authorization form (Fig. 16-9) should include the following:
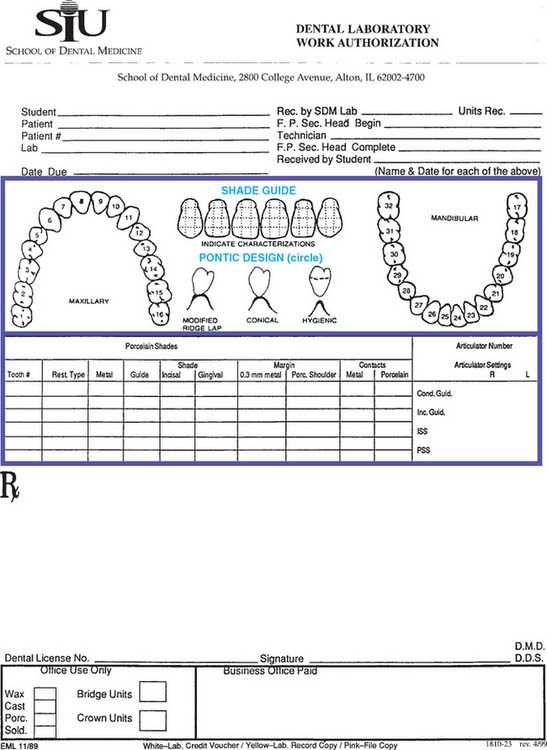
Fig. 16-9 Work authorization form. Cond. Guid., condylar guidance angle; Inc. Guid., incisal guidance; ISS, immediate side shift; Porc., porcelain; PSS, progressive side shift; SDM, School of Dental Medicine.
The dentist must be familiar with the materials that the technician prefers to use for certain procedures. Specifying those materials can save both time and effort. The technician should also respect the selection when the dentist requests a specific material. Written instructions should be explicit.17
Communication improves if the technician and dentist discuss a particular choice rather than if the dentist issues a bald statement written on the work authorization form. It may be inconvenient for the technician to comply with a request, and so its importance should be discussed.
Occlusion
The work authorization form should designate the location of the occlusal contacts. It must be specified whether they are to be on metal or porcelain. In theory, the two most desirable occlusal schemes are cusp-fossa and cusp-marginal ridge. Assuming that these will be attained in every case is unrealistic, however, because they can be accomplished consistently only when the opposing teeth are reasonably close to ideal relative positions (Angle Class I; see Chapter 1). Compromises often must be made, especially when teeth are being restored to conform to an existing dentition. For example, when a mandibular molar is in a buccolingual edge-to-edge posterior relationship with its antagonist, a decision must be made whether to restore the tooth in a reverse articulation or whether the tooth preparation should be modified (additional reduction of the buccal functional cusp bevel) to accommodate a more conventional occlusal relationship. As an alternative, restoring the opposing tooth may need to be considered.
If the dentist has performed a diagnostic tooth preparation and waxing (see Chapter 2), it is possible to communicate the desired occlusal relationship or tooth form very specifically (Fig. 16-10). A wax record rim that has been adjusted intraorally can convey a general idea of the desired position of the occlusal plane (Fig. 16-11). Similarly, a custom anterior guide table made by the dentist from anterior provisional restorations that have proved comfortable for the patient is most helpful to the technician in reproducing the same anterior guidance in the definitive fixed prostheses (Fig. 16-12). An impression of an interim crown poured in fast-setting dental stone is an excellent means of communicating the desired size and contours (Fig. 16-13). On occasion, when a single crown is to be made, an existing malocclusion may be accepted. This can limit the need for more extensive treatment, although it makes sense only if the opposing teeth will not need a restoration in the near future.
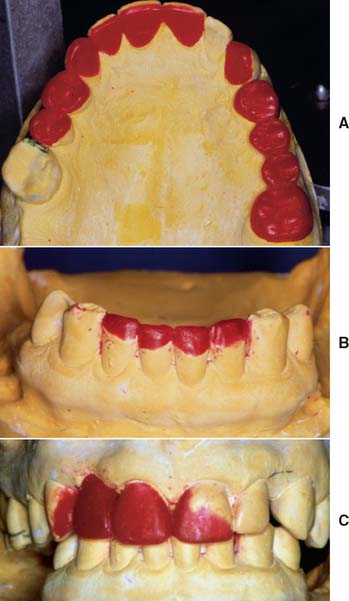
Fig. 16-10 Diagnostic waxing used to communicate desired occlusal form (A), the mandibular incisal edge position (B), and the shape of maxillary incisors (C).
(Courtesy of Dr. M. Chen.)

Fig. 16-11 A wax record rim that has been adjusted intraorally with a Fox plane can provide helpful information to the technician. Note that the desired position of the midline has been marked.

Fig. 16-12 A custom anterior guide table made from anterior provisional restorations that have proved comfortable for the patient: The guide table helps the technician replicate lingual contours in the fixed prostheses.

Fig. 16-13 A putty impression of the interim restorations has been poured. The resulting cast conveys desired tooth size and form and can be used as a starting point for contour waxing (see Chapter 19).
(Courtesy of Dr. M. Chen.)
Connectors
The work authorization form should specify which connectors are to be cast, which are to be preceramic soldered, and which are to be postceramic soldered. The sequence of the planned procedures should be indicated and discussed when necessary or when clarity can be enhanced. If nonrigid connectors are requested, the desired type of connector and path of placement should be specified.
Pontic and substructure design
Pontic design is discussed in Chapter 20. A simple checklist on the work authorization form should suffice if the dentist and technician have agreed on applicable expectations and requirements.17,18
The design of metal substructures for metal-ceramic restorations is somewhat controversial. Many technicians believe that it is not necessary to first create the contours of the completed restoration in wax and then cut back the veneering area. We disagree, and we present our reasoning in Chapter 19 (Fig. 16-14). The authorization should specify whether the anatomic contour wax patterns are to be returned for evaluation and possible modification. The more complex the restorative effort, the more crucial a careful evaluation becomes at this stage. Long-term success is the goal, and inadequate framework design is a relatively common cause of failure for which the dentist bears the responsibility (although the dentist often blames the ceramist).
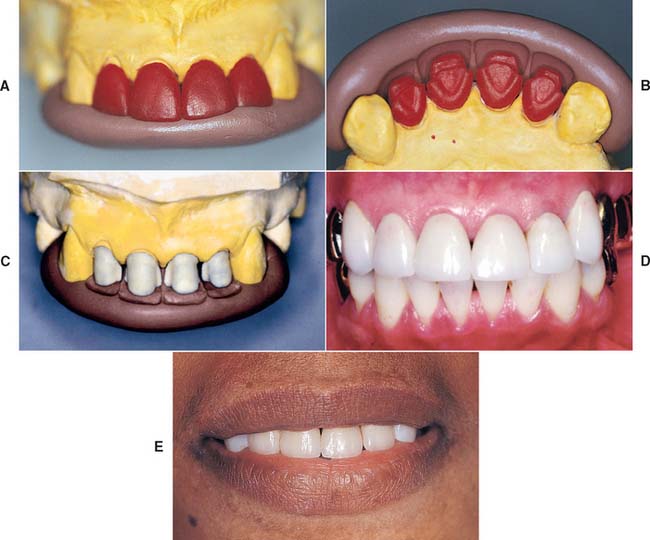
Fig. 16-14 Anatomic contour waxing (A) and cutback (B) with the use of incisal (A) and facial (B) polyvinyl siloxane indexes. C, The same indexes are used during porcelain application. D and E, The desired form is accurately replicated (D), and this leads to predictable success when esthetics are paramount (E).
Shade selection
With the prevalence of tooth-colored restorations, dentists and technicians have become acutely aware of the difficulty involved in communicating shade selection. A thorough understanding of the principles of color science (presented in Chapter 23) and of the use of internal and surface colorants (discussed in Chapters 24 and 30) is essential to both parties.
Many dentists and technicians have found a diagram of the tooth that allows specifications of multiple shades helpful (Fig. 16-15).19 The diagram should be large enough to designate a cervical shade, an incisal shade, and any applicable individual characterization. Diagrams on most preprinted laboratory prescription forms do not provide adequate space (see Fig. 16-9), and so other space must be available. A separate entry regarding the value or brightness can be helpful. When selecting a shade, the dentist should use a guide that corresponds to the ceramic system used by the technician. On occasion, it may not be possible to obtain a match with a simple shade guide (e.g., the Vita Lumin vacuum system). In those cases, an alternative guide or a shade distribution chart (outlined in Chapter 23) should be used. The dentist must have excellent color perception skills and should be able to precisely transfer those onto a written prescription that includes a large, detailed diagram that allows the ceramist to accurately reproduce the shade observed and described by the clinician. Close communication and cooperation are obviously necessary, and a trial porcelain firing may be needed.
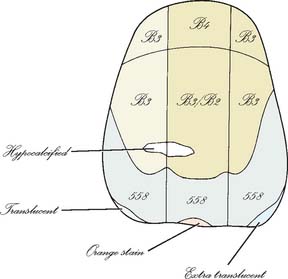
Fig. 16-15 A shade distribution chart must be adequate in size to permit inclusion of enough detail. Subtle differences observed in cervical shades are identified, as are surface details such as hypocalcification, incisal translucency, and stains.
A practical alternative to written color communication is the use of light-cured, resin-based staining kits to custom-stain a shade tab. The closest matching shade tab is selected and modified by stains mixed with liquid resin. Once the desired match has been obtained, the resin is light-cured, and the customized tab is sent to the dental laboratory. The ceramist then has an actual reference and can compare the work and make the required modifications, thus ensuring predictable success. A number of tooth shade–recording devices have been developed: colorimeters, spectrophotometers, and digital camera systems. (See also Chapter 23.) These techniques hold promise, although research on their reliability and reproducibility shows varying results with different shade guides. In general, color measurement reproducibility is better under controlled research laboratory setting than intraorally. Several of these systems provide a detailed color analysis in printed or electronic format (Fig. 16-16), which can be used to help communicate the specific shade or shades to the dental ceramist.
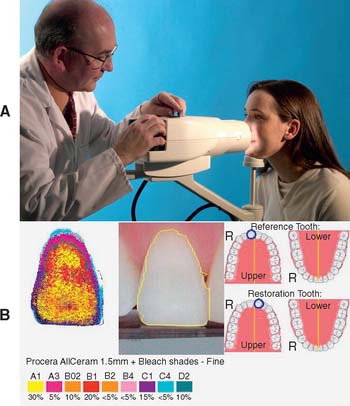
Fig. 16-16 Digital shade analysis. A, DCM Ikam digital camera with D-65 illumination. B, Example of analysis that is provided to assist the technician in development of the desired shade.
(Courtesy of Digital Colour Measurement Ltd., West Yorkshire, United Kingdom.)
If esthetic requirements are extensive or difficult to communicate through the means just described, involving dental laboratory personnel in the shade selection process may be helpful. The ADA takes the position that when a dentist requests the assistance of a dental laboratory technician in the shade selection process, this does not constitute the practice of dentistry by the technician, provided the activity is undertaken in consultation with the dentist and that it complies with the dentist’s written instructions. Specifically, the shade selection site, whether dental office or laboratory (where lawful), should be determined by the professional judgment of the dentist in the best interest of the patient and where communication between dentist, patient, and technician is enhanced.10
Additional information
Additional information often helps the technician considerably. Reference to diagnostic waxing can communicate specific information about desired tooth length and form or a desired occlusal arrangement. A custom anterior guide table (see Chapter 2) provides specific information to follow as anterior guidance is established in maxillary and/or mandibular anterior crowns. Casts of provisional restorations are invaluable to the technician when he or she is asked to fabricate fixed dental prostheses with a high esthetic requirement. They provide information about midlines, incisal edge position, and coronal form and are the most practical way of accurately conveying information to the laboratory (Fig. 16-17). The diagnostic waxing enables the dentist to explore all the treatment alternatives before choosing a course of therapy. A resin interim restoration can be fabricated and adjusted intraorally as necessary for optimum appearance and function. Standardized digital images can be especially helpful in conveying essential additional information.

Fig. 16-17 A, Diagnostic casts, anterior guide table, and waxing provide additional information for the technician. B and C, Carefully adjusted interim restorations are an essential part of complex rehabilitation. The 19-year-old patient had generalized hypoplastic amelogenesis imperfecta, rough pattern (type I F). Her interim restorations were duplicated and replicated in the definitive prosthesis.
(B and C, Courtesy of Dr. A. Hernandez.)
APPROPRIATE CHECKS
In any new working relationship between a dentist and a technician, every laboratory step should be reviewed in detail for the initial patients. Only then can teamwork develop over time. As the dentist and technician become familiar with each other’s preferences, several steps may then be combined.
The initial review may include the wax patterns for corrective shaping of occlusal and axial contours of retainers and pontics. When treating patients with fixed dental prostheses and metal-ceramic crowns, the dentist must decide whether the restorations should be completed through porcelain application in the laboratory or whether a preliminary metal substructure evaluation appointment is needed. We recommend routine evaluations of the metal substructure for metal-ceramic restorations (Fig. 16-18). As an example, the technician may not have adequate information to evaluate how far the veneering area should be extended into the cervical embrasures, and this can be readily determined by the dentist during evaluation. When fixed dental prostheses are soldered, often it is best to index the component parts directly in the mouth rather than rely on the accuracy of the definitive cast (Fig. 16-19). An evaluation appointment can facilitate making small corrections of discrepancies that could later become significant errors. Similarly, it may be advantageous to plan an evaluation appointment for final contouring, texturing, and characterization of a metal-ceramic restoration in the bisque bake, before glazing. It takes time and effort to perform these clinical procedures (see Chapter 30), but patients will recognize and appreciate the improved results.

Fig. 16-18 Unrealistic expectations by the dental technician. Inappropriate substructure design provides insufficient support for the porcelain veneer. This fixed dental prosthesis must be remade.

Fig. 16-19 Intraoral fabrication of an autopolymerizing resin soldering index that relates two components of a fixed dental prosthesis.
The use of checklists by both clinician and technician can be helpful.18,20 For instance, before an impression leaves the dental office, the dentist and auxiliary personnel can use a standard protocol to confirm that finish lines are distinct; that no blood or saliva is present in impressions; that disinfection protocols were followed; that no voids, tears, defects, or areas where the tray was seated are present; and that contact has not occurred between occlusal sur faces and the tray, creating thin spots that can lead to articulation errors. For casts, die trimming, the absence of undercuts, the retention form, the adequacy of reduction for facial porcelain and porcelain margins, and the occlusal clearance need to be confirmed.
Where retainers for partial removable dental prostheses are involved, the prescription and cast are checked to ensure availability of all pertinent information in relation to the path of insertion of the partial removable dental prosthesis, the guide planes, the rest seats, and the desired heights of contour (Fig. 16-20).

SUMMARY
The key to high-quality fixed prosthodontics lies in good communication between the dentist and the technician. All too often, each operates in a vacuum: The dentist forgets how a straightforward step such as rounding line angles can expedite the fabrication of a restoration, or the technician is unaware of the difficulties of a particular clinical phase (e.g., impression making or a remount procedure).
Through mutual respect and a coordinated effort, each can contribute to the delivery of patient care and at the same time keep failures to a minimum.
The most common problems seen by the dentist at evaluation are poor marginal adaptation, poor occlusion, poor axial contour (specifically, overcontouring of the cervical third of the tooth), and haphazard pontic and substructure design. The most common problems encountered by the technician are inadequate tooth reduction, “mystery margins,” improper articulation, and vagueness in color communication.
The use of certain ancillary devices (e.g., diagnostic waxing and casts of provisional restorations) helps both dentist and technician deliver more effective treatment to the prosthodontic patient.
The student and practitioner involved in fixed prosthodontic treatment must acquire an in-depth understanding of the laboratory procedures described in the following chapters in this section. Often such understanding is most rapidly developed by personal involvement in the technical aspects of clinical dentistry. Over time, this leads to significantly improved interaction with dental technicians, resulting in improved clinical decision making and more predictable and successful fixed prostheses.
 GLOSSARY*
GLOSSARY*
CDL: acronym for Certified Dental Laboratory
CDT: acronym for Certified Dental Technician
Certified Dental Laboratory: in the United States, a dental laboratory that has met established specific standards for personnel skills, laboratory facilities and infection control and is certified by The National Board for Certification of Dental Laboratories
Certified Dental Technician: in the United States, a dental technician who has met established specific standards and is certified by The National Board for Certification of Dental Laboratories
work authorization: a signed written order provided by the dentist to the dental laboratory detailing the work to be performed and specifying the materials to be used
STUDY QUESTIONS
1 NADL [National Association of Dental Laboratories]. Media Room. Available at: http://www.nadl.org/mediafacts.shtml. (accessed August 11, 2005).
2 Bennett Napier CAE (Executive Director, National Association of Dental Laboratories): Personal communication July 18, 2005.
3 Small BW. Laboratory communication for esthetic success. Gen Dent. 1998;46:566.
4 Gleghorn T. Improving communication with the laboratory when fabricating porcelain veneers. J Am Dent Assoc. 1997;128:1571.
5 Warden D. The dentist-laboratory relationship: a system for success. J Am Coll Dent. 2002;69:12.
6 Aquilino SA, Taylor TD. Prosthodontic laboratory and curriculum survey. III. Fixed prosthodontic laboratory survey. J Prosthet Dent. 1984;52:879.
7 Leith R, et al. Communication between dentists and laboratory technicians. J Ir Dent Assoc. 2000;46:5.
8 Lynch CD, Allen PF. Quality of written prescriptions and master impressions for fixed and removable prosthodontics: a comparative study. Br Dent J. 2005;198:17.
9 Landesman HM. Prosthodontics. Clinical practice—professional affairs. Review of the literature. J Prosthet Dent. 1990;64:252.
10 American Dental Association. Current Policies. Chicago: American Dental Association, 1954–2003;137-140.
11 U.S. Department of Health and Human Services, Public Health Service. Recommended infection control practices for dentistry. MMWR. 1986;35:237.
12 Infection control recommendations for the dental office and the dental laboratory. Council on Dental Materials, Instruments, and Equipment. Council on Dental Practice. Council on Dental Therapeutics. J Am Dent Assoc. 1988;116:241.
13 Powell GL, et al. The presence and identification of organisms transmitted to dental laboratories. J Prosthet Dent. 1990;64:235.
14 Jorgenson MW, Goodkind RJ. Spectrophotometric study of five porcelain shades relative to dimensions of color, porcelain thickness, and repeated firings. J Prosthet Dent. 1979;42:96.
15 Leeper SH. Dentist and laboratory: a “love-hate” relationship. Dent Clin North Am. 1979;23:87.
16 Olin PS, et al. Current prosthodontic practice: a dental laboratory survey. J Prosthet Dent. 1989;61:742.
17 Drago CJ. Clinical and laboratory parameters in fixed prosthodontic treatment. J Prosthet Dent. 1996;76:233.
18 Deyton G. Communications checksheet will ease relations with laboratories. Mo Dent J. 1994;74(5):32.
19 Pensler AV. Shade selection: problems and solutions. Compendium Contin Educ Dent. 1998;19:387.
20 Maxson BB. Quality assurance for the laboratory aspects of prosthodontic treatment. J Prosthodont. 1997;6:204.