Chapter 1 Principles of radiography
Chapter contents
1.1 Aim
This chapter considers the basic principles of diagnostic radiography, therapeutic radiography and radiation protection. This should allow the reader to appreciate how the individual chapters within the text form part of a whole study.
1.2 Diagnostic and therapeutic radiography
X-rays (and other forms of radiation) can have two main uses in medicine. They can be used to investigate the patient’s illness or physical state through the production of an image – this forms the basis of diagnostic radiography; or they can be used to eliminate unwanted abnormal cells in certain body tissues – the basis of therapeutic radiography.
1.2.1 Diagnostic radiography
In diagnostic radiography, an image of structures within the patient’s body is produced on an image receptor or a monitor screen. Normally, of course, we cannot see inside each other’s bodies because light photons, to which our eyes are sensitive, are absorbed and reflected very close to the surface of body tissues.
To examine internal body structures using light, an instrument called an endoscope must be inserted into the body. This consists of fibre optic bundles which transmit the light to and from the region of interest and so allows the operator to view the organ. Such techniques are used in ‘keyhole surgery’. This type of imaging does carry some risk, or it may be uncomfortable for the patient, and so radiography will often be considered as an alternative.
Figure 1.1 shows a radiographer preparing the equipment for a common X-ray diagnostic examination.
As light is a form of electromagnetic radiation (see Ch. 17) and it seems logical to suggest that if we can take photons of electromagnetic radiation which have higher energies than light photons, then these may have sufficient energy to penetrate body tissues and allow us to visualize internal organs. X-rays are in this part of the electromagnetic spectrum and so will penetrate body tissues and allow us to image internal organs. Unfortunately the retina of the eye cannot detect X-rays and so we cannot see an image of a structure just by directing an X-ray beam on it. This means that the X-rays, which have passed through the body, must be made to strike an image receptor that will produce a visible image, for example an imaging plate.
The principal interactions involved in the basic requirements for the formation of a radiographic image are shown in Figure 1.2.
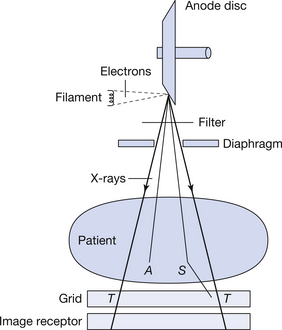
Figure 1.2 The principal interactions involved in the production of a radiographic image. A represents absorbed photons, S represents scattered photons and T represents transmitted photons.
X-rays are produced in the X-ray tube by accelerating electrons and causing these to collide with the target of the X-ray tube. To understand how this works we need to know about energy (see Ch. 4) and electricity (see Chs 7 and 11) as well as the construction of the X-ray transformer and X-ray tube (see Chs 14 and 30). The X-rays so produced are over a wide band of energies. Most of the photons that have insufficient energy to be of diagnostic value are removed from the beam using filtration (see Ch. 22) and the area of the patient irradiated is restricted using a diaphragm (see Ch. 25). The beam now interacts with the patient and a number of things may happen to the X-ray photons. These may be:
• transmitted (T in Fig. 1.2): these photons pass through the patient without interacting with the patient’s tissues. They are thus unaffected by their passage through the patient
• absorbed (A in Fig. 1.2): these photons interact with the patient’s tissues and as a result lose all of their energy. As the photon consists only of energy, then these photons disappear from the spectrum of radiation transmitted through the patient
• scattered (S in Fig. 1.2): these photons interact with the patient’s tissues and are then deflected from their original path. Such a deflection may or may not result in a loss of some of the photons’ energy.
Different tissues will absorb different amounts of radiation (see Ch. 25) and so a differentiated radiation pattern leaves the patient. The scattered radiation is not helpful to the image, so when the scatter production is significant, as much as possible of this is removed using a secondary radiation grid (see Ch. 25). Finally, the radiation interacts with the image receptor, where it is ‘captured’ and passed into a digital imaging system (see Ch. 34).
Radiographers employ other radiations in the course of their clinical work. Magnetic resonance imaging (MRI; see Ch. 39) makes use of powerful magnetic fields as well as radiofrequency waves. Both of these are examples of non-ionizing radiations, which are not thought to cause cancers but can have other biological effects on the human body. Radiofrequency waves are a form of electromagnetic radiation, just like X-rays, but have a much lower frequency. As a result they are much less energetic and fit lower down the electromagnetic spectrum. Ultrasound (see Ch. 42) is another example of a non-ionizing radiation used in radiography. But unlike X-rays and radiofrequency waves, ultrasound needs a medium like fluid or body tissue to pass through. This is because it consists of a series of vibrations passing through molecules and is not a form of electromagnetic radiation. Sound cannot be heard in a vacuum. But X-rays, radio waves and light, which are all electromagnetic, can pass freely through outer space. Sound waves travel at different speeds in different body tissues, whereas X-rays always travel at the same extremely high speed, which is termed the ‘speed of light’– about 300 000 kilometers per second!
1.2.2 Therapeutic radiography
In therapeutic radiography, we are not trying to produce images but are using the biological effects of radiation to kill tumour cells. At the same time, we try to cause as little damage as possible to the healthy cells in the body.
There are four main methods of cancer treatment: surgery, chemotherapy, alteration of the hormone balance and radiotherapy. They may be used in isolation or together to give the optimum treatment regime for a given cancer in a given patient. The treatment may be radical or palliative. The former is an all-out effort to achieve a cure and the latter is used to relieve pain and other distressing symptoms when no cure for the disease is possible. This is normally in the terminal stages of the disease.
The relative success of radiotherapy in the management of cancer lies in the fact that malignant cells are more sensitive to radiation than healthy cells in the same organ. The reasons for this will be discussed in Chapter 25. In spite of this, a number of healthy cells are affected by radiation and so must be given time to recover. Thus the radiation dose is delivered as a number of treatments rather than as a single dose. This technique is known as fractionation and may mean that a patient has 15–30 treatments over a period of 3–6 weeks.
1.3 Methods of radiation treatment
A detailed description of the different methods of radiation treatment is beyond the scope of this introductory chapter and the reader is directed to some of the more specialized texts on the subject. In considering the overview of radiation treatment methods, we can, however, identify some distinct types, which we will discuss further. These are:
1.3.1 Teletherapy
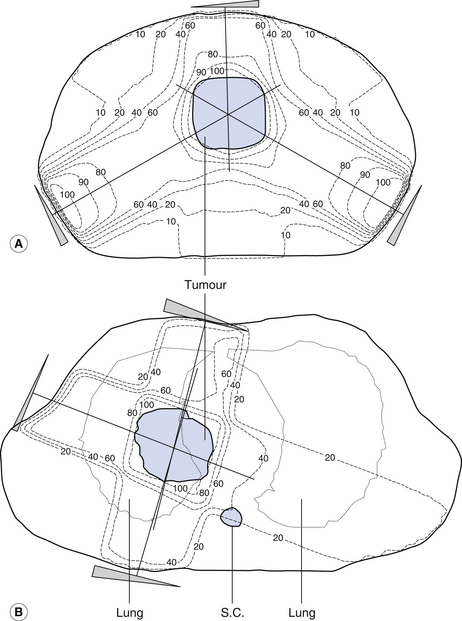
Here an external source of radiation (normally X-rays or gamma rays) is directed at the tumour. The aim is to give the maximum dose to the tumour and the minimum dose to the healthy tissue. This is often achieved by treating the tumour with a number of fields (see Fig. 1.3). The areas in the patient that receive doses of equal value are joined by lines called isodose lines. The shape and the position of these lines may be altered by the use of absorbing wedges and compensators and also by altering the energy and shape of the treatment beam. Once the treatment plan has been produced, the positions of the treatment fields on the patient are checked in a simulator where the treatment angles can be set up and the fields marked. In areas of the patient around the head and the neck, accurate positioning and immobilization are achieved by placing this part in a specially prepared clear plastic shell.
1.3.2 Brachytherapy
When we use external radiation beams, the radiation must travel through healthy tissue to reach the tumour. There are some situations where tumours are relatively accessible from the body surface or are in body cavities where sealed radioactive sources (see Ch. 19) may be inserted. This technique is known as brachytherapy. The technique can often mean that a large dose can be delivered to the tumour while a much smaller dose strikes the surrounding tissues because of the effects of the inverse square law (see Ch. 26). If the sources were implanted directly by the radiotherapist, the dose to the hands of the operator could be quite large. This is overcome by inserting a number of guides into the correct position and mechanically inserting the sources over the guides for the required treatment. This technique is called afterloading and is often used in the treatment of pelvic cancers.
1.3.3 Nuclear medicine
A third possibility is that the radiation can be delivered to the tissue by allowing the tissue to absorb a certain radionuclide (see Ch. 19). This is probably best illustrated by considering the treatment of an overactive thyroid gland. The activity of the gland can be reduced by surgical removal of part of the gland, or some of its tissue may be destroyed using radiation. To allow the thyroid to produce the required hormones, it must absorb iodine. The patient may be given sodium iodide (where the iodine is in the form of 131I) as a capsule or in an oral solution. Some of this isotope (see Ch. 19) is taken up by the gland and the rest is secreted in the urine. 131I is a beta particle emitter (see Ch. 19) and this results in a radiation dose to the thyroid tissue, which reduces its metabolic rate to normal. Because of the limited range of the beta particles produced, there is less radiation dose to structures around the thyroid than there would be if we used an external radiation beam. 131I also has a relatively short half-life(8 days) (see Ch. 19) and so the radiation hazard posed by the patient to others can be minimized.
1.4 Radiation protection
All ionizing radiation of the cells which make up our bodies carries a risk of damage to those cells. It is also true that some tissues are more sensitive to radiation than others (see Ch. 44). The use of ionizing radiation in medicine is of great value to humans, but it is the largest single factor which contributes to the artificial radiation dose received by the human race. The contribution of the various radiation sources is shown in Figure 1.4.
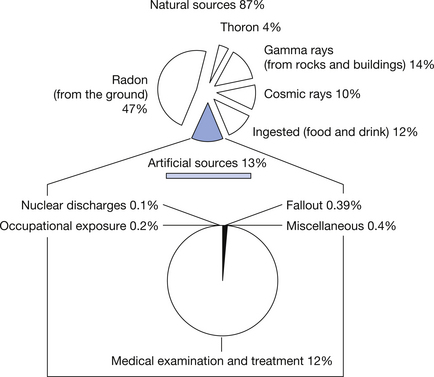
Figure 1.4 Sources of radiation exposure to humans.
(Based on data from the radiation section of the Health Protection Agency (formerly the National Radiological Protection Board.)
Because of this, we have a duty to minimize the dose to our patients and colleagues and so minimize the risk of radiation damage. The radiation dose is composed of primary radiation and secondary radiation, and so we need to look at the ways in which these are produced and absorbed. This will be considered in Chapter 44. Because of the known hazards of radiation, there are certain statutory requirements for radiation protection and monitoring in diagnostic and therapy departments (see Ch. 44). In terms of assessing the risk, it is important to know the dose received by both patients and radiation workers and this will be discussed in Chapter 27, which deals with the topic of radiation dosimetry.
Further reading
This overview covers a very large subject area and so only the principal texts are identified. Further reading in specialized topics will be covered in the chapter bibliographies.
Diagnostic radiography
Moores B.M., Wall B.F., Stieve S.E., et al. Optimisation of Image Quality and Patient Exposure in Diagnostic Imaging. London: British Institute of Radiology, 1989. British Institute of Radiology Report 18
Therapeutic radiography
Bomford C.K. Walter’s and Miller’s textbook of radiotherapy. Edinburgh: Churchill Livingstone, 1993.
Souhami R., Tobias J. Cancer and its Management. Oxford: Blackwell Scientific, 1987.
Wang C.C. Clinical Radiation Oncology: Indications, Techniques and Results, Second edn. New York: Wiley, 2000.
Radiation protection
Dowd S.B., Tildon E.R. Practical Radiation Protection and Applied Radiobiology, Second edn. Philadelphia: WB Saunders, 1999.
Statutory Instrument 1999/3232 The ionising radiation regulations, 1999. HMSO, London.
UK National Radiation Protection Division. (http://www.hpa.org.uk/radiation).