The general principles of physical examination
Students beginning their training in physical examination will be surprised at the formal way this examination is taught and performed.1,2 There are, however, a number of reasons for this formal approach. The first is that it ensures the examination is thorough and that important signs are not overlooked because of a haphazard method.3 The second is that the most convenient methods of examining patients in bed, and for particular conditions in various other postures, have evolved with time. By convention, patients are usually examined from the right side of the bed, even though this may be more convenient only for right-handed people. When students learn this, they often feel safer huddling on the left side of the bed with their colleagues in tutorial groups, but many tutors are aware of this strategy, particularly when they notice all students standing as far away from the right side of the bed as possible.
It should be pointed out here that there is only limited evidence-based information concerning the validity of clinical signs. Many parts of the physical examination are performed as a matter of tradition. As students develop their examination skills, experience and new evidence-based data will help them to refine their use of examination techniques. We have included information about the established usefulness of signs where it is available, but have also included signs that students will be expected to know about despite their unproven value.
This formal approach to the physical examination leads to the examination of the parts of the body by body system. For example, examination of the cardiovascular system, which includes the heart and all the major accessible blood vessels, begins with positioning the patient correctly. This is followed by a quick general inspection and then, rather surprisingly for the uninitiated, seemingly prolonged study of the patient’s fingernails. From there, a set series of manoeuvres brings the doctor to the heart. This type of approach applies to all major systems, and is designed to discover peripheral signs of disease in the system under scrutiny. The attention of the examining doctor is directed particularly towards those systems identified in the history as possibly being diseased, but of course proper physical examination requires that all the systems be examined.
The danger of a systematic approach is that time is not taken to stand back and look at the patient’s general appearance, which may give many clues to the diagnosis. Doctors must be observant, like a detective (Conan Doyle based his character Sherlock Holmes on an outstanding Scottish surgeon).4 Taking the time to make an appraisal of the patient’s general appearance, including the face, hands and body, conveys the impression to the patient (and to the examiners) that the doctor or student is interested in the person as much as the disease. This general appraisal usually occurs at the bedside when patients are in hospital, but for patients seen in the consulting room it should begin as the patient walks into the room and during the history taking, and continue at the start of the physical examination.
Diagnosis has been defined as ‘the crucial process that labels patients and classifies their illnesses, that identifies (and sometimes seals) their likely fates or prognoses and that propels us towards specific treatments in the confidence (often unfounded) that they will do more good than harm’.5
In normal clinical practice, the detail of the physical examination performed will be ‘targeted’ and will depend on clues from the history and whether the consultation is a follow-up or new consultation. Students, however, must know how to perform a complete examination of the body systems, even though they will not often perform this in practice.
Clinical examination
In clinical examinations you will be expected to be able to demonstrate a polished and thorough examination method—this book will teach you how. The most common examination format is the objective structured clinical examination (OSCE), which is discussed later in this chapter. Other formats used include the long case (testing your ability to take the history, perform a thorough examination and plan management, just as people do in clinical practice) and the short case (testing your ability to examine a specific part or system and your diagnostic skills, without knowing the details of the history—not an easy task).
A high level of competency in history taking and physical examination remains central to the provision of effective and safe medical practice. Learn, practise and hone these core skills every day.
How to start
A few simple steps will help put the patient at ease and assist you in completing the examination (see Text box 3.1). Always wash your hands before and after, to protect the patient and yourself. Try to examine in a warm room that has good lighting so that you maximise your chances of seeing the signs. Introduce yourself and seek the patient’s permission to examine him or her. For an examination of the genital or anal areas, ask whether the patient would like a chaperone (and include the chaperone’s name in the records, if you use one). Unless the adult patient requests that relatives stay, ask them to leave temporarily. Make sure the patient is positioned comfortably and adequately exposed (but not over exposed—cover or recover areas not being directly examined). Start by standing on the right side of the bed. Be gentle and courteous.
First impressions
First impressions of a patient’s condition must be deliberately sought. Make a conscious point of assessing the patient’s general condition right at the start. The specific changes that occur in particular illnesses (e.g. myxoedema) will be discussed in detail in the appropriate chapters. However, certain abnormalities should be obvious to the trained or training doctor.
First, decide how sick the patient seems to be: that is, does he or she look generally ill or well? The cheerful person sitting up in bed reading Proust (see Figure 3.1) is unlikely to require urgent attention to save his life. At the other extreme, the patient on the verge of death may be described as in extremis or moribund. In this case the patient may be lying still in bed and seem unaware of the surroundings. The face may be sunken and expressionless, and respiration may be shallow and laboured; at the end of life, respiration often becomes slow and intermittent, with longer and longer pauses between rattling breaths.
When a patient walks into the consulting room or undresses for the examination, there is an opportunity to look for problems with mobility and breathlessness. Apart from gaining a general impression of a patient’s state of health, certain general physical signs must be sought.
VITAL SIGNS
Certain important measurements must be made during the assessment of the patient. These relate primarily to cardiac and respiratory function and comprise:
For example, an increasing respiratory rate has been shown to be an accurate predictor of respiratory failure.6 Patients in hospital may have continuous ECG and pulse oximetry monitoring on display on a monitor; these measurements may be considered an extension of the physical examination.
The vital signs must be assessed at once if a patient appears unwell. Patients in hospital have these measurements taken regularly and charted. They provide important basic physiological information.
Facies
A specific diagnosis can sometimes be made by inspecting the face, its appearance giving a clue to the likely diagnosis. Other physical signs must usually be sought to confirm the diagnosis. Some facial characteristics are so typical of certain diseases that they immediately suggest the diagnosis and are called the diagnostic facies (the Latin word facies means more than just face, including form, shape, appearance and character; see List 3.1 and Figures 3.2–3.7). Apart from these ‘spot diagnoses’, there are several other important abnormalities that must be looked for in the face.
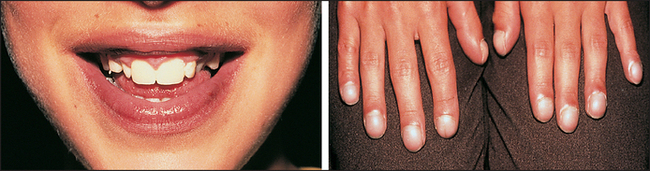
Figure 3.2 Cyanosis (From Zitelli BJ, Davis HW. Atlas of pediatric physical diagnosis, 5th edn. Elsevier, 2007.

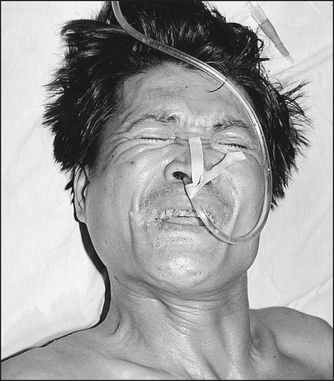
Figure 3.4 Risus sardonicus (tetanus) (From Cook GC. Manson’s tropical diseases, 22nd edn. Saunders, 2008)

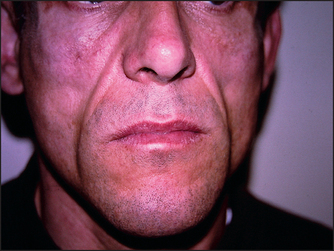
Figure 3.6 Lipodystrophic facies (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)

Figure 3.7 Some neurological diagnostic facies: (a) myopathic; (b) myotonic (From Mir MA, Atlas of clinical diagnosis, 2nd edn. Edinburgh: Saunders, 2003, with permission.)
JAUNDICE
When the serum bilirubin level rises to about twice the upper limit of normal, bilirubin is deposited in the tissues of the body. It then causes yellow discolouration of the skin (jaundice) and, more dramatically, the apparent discolouration of the sclerae. The usual term scleral icterus is misleading, since the bilirubin is actually deposited in the vascular conjunctiva rather than the avascular sclerae. The sclerae (conjunctivae) are rarely affected by other pigment changes. In fact, jaundice is the only condition causing yellow sclerae. Other causes of yellow discolouration of the skin, but where the sclerae remain normal, are carotenaemia (usually due to excess consumption of carotene, often from intemperate eating of carrots or mangoes), acriflavine, fluorescein and picric acid ingestion.
Jaundice may be the result of excess production of bilirubin, usually from excessive destruction of red blood cells (termed haemolytic anaemia), when it can produce a pale lemon-yellow scleral discolouration. Alternatively, jaundice may be due to obstruction of bile flow from the liver, which, if severe, produces a dark-yellow or orange tint. Scratch marks may be prominent due to associated itching (pruritus). The other main cause of jaundice is hepatocellular failure. Gilbert’s disease is also a common cause of jaundice.a It causes a mild elevation of unconjugated bilirubin and is due to an inherited enzyme deficiency that limits bilirubin conjugation; it has a benign prognosis. Jaundice is discussed in detail on page 179.
CYANOSIS
This refers to a blue discolouration of the skin and mucous membranes (see Figure 3.2); it is due to the presence of deoxygenated haemoglobin in superficial blood vessels. The haemoglobin molecules change colour from blue to red when oxygen is added to them in the lungs. If more than about 50 g/L of deoxygenated haemoglobin is present in the capillary blood, the skin will have a bluish tinge.7 Cyanosis does not occur in anaemic hypoxia because the total haemoglobin content is low. Cyanosis is more easily detected in fluorescent light than in daylight.
Central cyanosis means that there is an abnormal amount of deoxygenated haemoglobin in the arteries and that a blue discolouration is present in parts of the body with a good circulation, such as the tongue. This must be distinguished from peripheral cyanosis, which occurs when the blood supply to a certain part of the body is reduced and the tissues extract more oxygen than normal from the circulating blood: for example, the lips are often blue in cold weather, but the tongue is spared. The presence of central cyanosis should lead to a careful examination of the cardiovascular (Chapter 5) and respiratory (Chapter 10) systems (see also List 3.2).
PALLOR
A deficiency of haemoglobin (anaemia) can produce pallor of the skin and should be noticeable, especially in the mucous membranes of the sclerae if the anaemia is severe (less than 70 g/L of haemoglobin). Pull the lower eyelid down and compare the colour of the anterior part of the palpebral conjunctiva (attached to the inner surface of the eyelid) with the posterior part where it reflects off the sclera. There is usually a marked difference between the red anterior and creamy posterior parts (see Figure 38.4 on page 510). This difference is absent when significant anaemia is present. Although this is at best a crude way of screening for anaemia, it can be specific (though not sensitive) when anaemia is suspected for other reasons. It should be emphasised that pallor is a sign, while anaemia is a diagnosis based on laboratory results.
Facial pallor may also be found in shock, which is usually defined as a reduction of cardiac output such that the oxygen demands of the tissues are not being met (see List 3.3). These patients usually appear clammy and cold and are significantly hypotensive (have low blood pressure). Pallor may also be a normal variant due to a deep-lying venous system and opaque skin.
HAIR
Bearded or bald women and hairless men not uncommonly present to doctors. These conditions may be a result of more than the rich normal variations of life, and occasionally are due to endocrine disease (see Chapter 29).
Weight, body habitus and posture
Look specifically for obesity. Note the fat distribution: is the patient apple (abdominal obesity) or pear shaped (generalised obesity including hips and thighs)? Obesity is most objectively assessed by calculating the body mass index (BMI), whereby the patient’s weight in kilograms is divided by the height in metres squared. Normal is less than 25 kg/m2. A BMI of ≥30 indicates frank obesity; morbid obesity is a BMI >40. Medical risks are increasingly recognised in association with obesity (see List 3.4).
There are racial differences in BMI associated with medical risk. Certain races (e.g. Australian Aboriginals, Asians) have an increased medical risk once the BMI reaches 23 (and obesity is defined as a BMI of 25 or higher).
The waist–hip ratio (WHR) is also predictive of health risk. This measurement is of the circumference of the waist (at the midpoint between the costal margin and the iliac crest) divided by that at the hips (at the widest part around the buttocks). Increased risk occurs when this exceeds 1.0 for men and 0.85 for women. Simple waist measurement correlates with the risks of obesity. A waist circumference of more than 80 centimetres for females and 94 centimetres for males indicates an increased risk and more than 88 centimetres for females and 102 centimetres for males indicates a greatly increased risk. These measurements can usefully be made repeatedly and recorded.
Severe underweight (BMI <18.5) is called cachexia.8 Look for wasting of the muscles, which may be due to neurological or debilitating disease, such as malignancy. There may be signs of vitamin deficiencies described later in this book (pages 226 and 277). For example, vitamin C deficiency causes scurvy, which is characterised by small bleeds around the hair follicles (perifollicular haemorrhages; see Figure 3.8) as well as bruising. Vitamin K deficiency also causes bruising but not perifollicular haemorrhages.

Figure 3.8 Scurvy with perifollicular haemorrhages (From Color atlas of clinical hematology. Mosby, 2010.)
Note excessively short or tall stature, which may be rather difficult to judge when the patient is lying in bed. Inspect for limb deformity or missing limbs (rather embarrassing if missed in viva examinations) and observe whether the physique is consistent with the patient’s stated chronological age. A number of body shapes are almost diagnostic of different conditions (see List 3.5). If the patient walks into the examining room, the opportunity to examine gait should not be lost: the full testing of gait is described in Chapter 34.
Hydration
Although this is not easy to assess, all doctors must be able to estimate the approximate state of hydration of a patient.9–11 For example, a severely dehydrated patient is at risk of death from developing acute renal failure, while an overhydrated patient may develop fluid overload and pulmonary oedema. Excessive oral rehydration with water (e.g. during sporting events) can lead to reduced blood sodium levels and cause confusion and even loss of consciousness.
For a traditional assessment of dehydration (see List 3.6), inspect for sunken orbits, dry mucous membranes and the moribund appearance of severe dehydration. Reduced skin turgor (pinch the skin: normal skin returns immediately on being released) occurs in moderate and severe dehydration (this traditional test is not of proven value, especially in the elderly, whose skin may always be like that). The presence of dry axillae increases the likelihood of dehydration and a moist tongue reduces the likelihood, but look for a combination of signs for guidance.
Take the blood pressure and look for a fall in pressure when the patient sits or stands up after lying down. The patient should stand, if possible, for at least 1 minute before the blood pressure is taken again (the patient’s inability to stand because of postural dizziness is probably a more important sign than the blood pressure difference). This is called postural hypotension. An increase in the pulse rate of 30 bpm or more, when the patient stands, is also a sign of hypovolaemia.
Weigh the patient. Following the body weight daily is the best way to determine changes in hydration over time. For example, a 5% decrease in body weight over 24 hours indicates that about 5% of body water has been lost (use the same set of scales).
Assessment of the patient’s jugular venous pressure is one of the most sensitive ways of judging intravascular volume overload, or overhydration (see Chapter 5).
The hands and nails
Changes occur in the hands in many different diseases (see Figures 3.9–3.12). It is useful as an introduction to shake a patient’s hand when meeting him or her. Apart from being polite, this may help make the diagnosis of dystrophia myotonica, a rare muscle disease in which the patient may be unable to let go. Shaking hands is also an acceptable and gentle way of introducing the physical examination. The physical examination is an intrusive event that is tolerated only because of the doctor’s (and even the medical student’s) professional and cultural standing.

Figure 3.9 Onychogryphosis: finger or toe nails shaped like a talon. This deformity is due to repeated trauma or candida infection. The name derives from the mythological animal the griffin, which had the head, body and tail of a lion and an eagle’s head, wings and talons. (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)

Figure 3.10 Beau’s lines (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)

Figure 3.11 (a) and (b) Systemic lupus erythematosus (Zitelli BJ, McIntire SC, Nowalk AJ. Zitelli and Davis’ Atlas of Pediatric Physical Diagnosis, 6th ed, Saunders, 2012.)

Examination of the hands by looking, feeling and moving is the gateway to diagnosis in many cases. There is no subspecialty of internal medicine in which examination of the hands is not rewarding. The shape of the nails may change in some cardiac and respiratory diseases, the whole size of the hand may increase in growth hormone excess (acromegaly; page 364), gross distortion of the hands’ architecture occurs in some forms of arthritis (page 347), tremor or muscle wasting may represent neurological disease and pallor of the palmar creases may indicate anaemia (see Table 3.1). Yellow tar staining of the fingers indicates a cigarette smoker (see Figure 3.12). These and other changes in the hands await you later in the book.
TABLE 3.1
Nails signs in systemic disease
| Nail sign | Some causes | Page no. |
| Blue nails | Cyanosis, Wilson’s disease, ochronosis | 30 |
| Red nails | Polycythaemia (reddish-blue), carbon monoxide poisoning (cherry-red) | 284 |
| Yellow nails | Yellow nail syndrome | 154 |
| Clubbing | Lung cancer, chronic pulmonary suppuration, infective endocarditis, cyanotic heart disease, congenital, HIV infection, chronic inflammatory bowel disease etc | 63 |
| Splinter haemorrhages | Infective endocarditis, vasculitis | 63 |
| Koilonychia (spoon-shaped nails) | Iron deficiency, fungal infection, Raynaud’s disease | 270 |
| Onycholysis | Thyrotoxicosis, psoriasis, over-enthusiastic cleaning beneath the nails (quite common) | 359 |
| Non-pigmented transverse bands in the nail bed (Beau’s lines;* see Figure 3.10) | Fever, cachexia, malnutrition | 36 |
| Leuconychia (white nails) | Hypoalbuminaemia | 187 |
| Transverse opaque white bands (Muehrcke’s lines) | Trauma, acute illness, hypoalbuminaemia (also caused by chemotherapy) | 246 |
| Single transverse white band (Mees’ lines) | Arsenic poisoning, renal failure (also caused by chemotherapy or severe illness) | 249 |
| Nail fold erythema and telangiectasia | Systemic lupus erythematosus | 331 |
| ’Half and half nails’ (proximal portion white to pink and distal portion red or brown: Terry’s nails) | Chronic renal failure, cirrhosis | 187 |
*Joseph Honoré Simon Beau (1806-1865) first described this in 1846. The cause of Beau’s lines is usually a serious systemic illness or treatment (e.g. septicaemia or chemotherapy), which stops growth of the nail plate. After recovery the nail grows again. The distance of the line from the cuticle can be measured to work out when the illness occurred. The finger nail plate grows at an average rate of 0.1 mm/day.
Temperature
The patient’s temperature should always be recorded as part of the initial clinical examination. The normal temperature (in the mouth) ranges from 36.6°C to 37.2°C (98°F to 99°F) (see Table 3.2). The rectal temperature is normally higher and the axillary and tympanic temperatures are lower than the oral temperature (see Table 3.2). In very hot weather the temperature may rise by up to 0.5°C. Patients who report they have a fever are usually correct, as is a mother who reports that her child’s forehead is warm and that fever is present.
TABLE 3.2
| Normal | Fever | |
| Mouth | 36.8°C | >37.3°C |
| Axilla* | 36.4°C | >36.9°C |
| Rectum | 37.3°C | >37.7°C |
There is a diurnal variation; body temperature is lowest in the morning and reaches a peak between 6 pm and 10 pm. The febrile pattern of most diseases follows this diurnal variation. The pattern of the fever (pyrexia) may be helpful in diagnosis (see Table 3.3).
TABLE 3.3
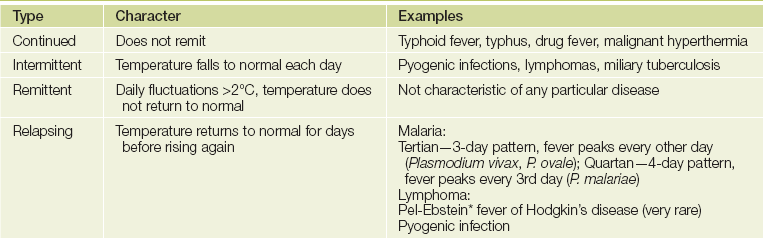
Note: The use of antipyretic and antibiotic drugs has made these patterns unusual today.
*Pieter Pel (1859-1919), Professor of Medicine, Amsterdam; Wilhelm Ebstein (1836-1912), German physician
Very high temperatures (hyperpyrexia, defined as above 41.6°C) are a serious problem and may result in death. The causes include heat stroke from exposure or excessive exertion (e.g. in marathon runners), malignant hyperthermia (a group of rare genetically determined disorders in which hyperpyrexia occurs in response to various anaesthetic agents [e.g. halothane] or muscle relaxants [e.g. suxamethonium]), the neuroleptic malignant syndrome (a reaction to antipsychotic medication) and hypothalamic disease.
Hypothermia is defined as a temperature of less than 35°C. Normal thermometers do not record below 35°C and therefore special low-reading thermometers must be used if hypothermia is suspected. Causes of hypothermia include hypothyroidism and prolonged exposure to cold.
Smell
Certain medical conditions are associated with a characteristic odour.12 These include the sickly sweet acetone smell of the breath of patients with ketoacidosis, the sweet smell of the breath in patients with liver failure, the ammoniacal fish breath (‘uraemic fetor’) of kidney failure and, of course, the stale cigarette smell of the patient who smokes. This smell will be on his or her clothes and even on the referral letter kept in a bag or pocket next to a packet of cigarettes. Recent consumption of alcoholic drinks may be obvious. ‘Bad breath’, although often of uncertain cause, may be related to poor dental hygiene, gingivitis (infection of the gums) or nasopharyngeal tumours. Chronic suppurative infections of the lung can make the breath and saliva foul-smelling. Skin abscesses may be very offensive, especially if caused by anaerobic organisms or Pseudomonas spp. Urinary incontinence is associated with the characteristic smell of stale urine, which is often more offensive if the patient has a urinary tract infection. The smell of bacterial vaginosis is usually just described as offensive. Severe bowel obstruction and the rare gastrocolic fistula can cause faecal contamination of the breath when the patient belches. The black faeces (melaena) caused by upper gastrointestinal bleeding and the breakdown of blood in the gut has a strong smell, familiar to anyone who has worked in a gastroenterology ward. The metallic smell of fresh blood, sometimes detectable during invasive cardiological procedures, is very mild by comparison.
Preparing the patient for examination
An accurate physical examination is best performed when the examining conditions are ideal. This means that, if possible, the patient should be in a well-lit room (preferably daylight) from which distracting noises and interruptions have been excluded (rarely possible in busy hospital wards). Screens must be drawn around patients before the examination. Consulting rooms and outpatient clinics should be set up to ensure privacy and comfort for patients.
Patients have a right to expect that students and doctors will have washed their hands or rubbed them with antimicrobial hand sanitisers before they perform an examination. This is as important in clinics and surgeries as in hospital wards. Many hospitals now have notices telling patients that they may ask their doctors if their hands have been washed. The diaphragm and bell of the stethoscope should be cleaned with an antimicrobial wipe and any other equipment that touches a patient should be disposable (e.g. neurology pin) or wiped down.
The examination should not begin until permission has been asked of the patient and the nature of the examination has been explained.
The patient must be undressed so that the parts to be examined are accessible. Modesty requires that a woman’s breasts be covered temporarily with a towel or sheet while other parts of the body are being examined. Male doctors and students should be accompanied by a female chaperone when they examine a woman’s pelvis, rectum or breasts. Both men and women should have the groin covered, for example, during examination of the legs. Outpatients should be provided with a gown to wear. However, important physical signs will be missed in some patients if excessive attention is paid to modesty.
The position of the patient in bed or elsewhere should depend on what system is to be examined. For example, a patient’s abdomen is best examined if he or she lies flat with one pillow placed so that the abdominal muscles are relaxed. This is discussed in detail in subsequent chapters.
Within each of the examining systems, four elements comprise the main parts of the physical examination: looking—inspection; feeling—palpation; tapping—percussion; and listening—auscultation.b For many systems a fifth element, assessment of function, is added. Measuring is also relevant in some systems. Each of these is discussed in detail in the following chapters.
Evidence-based clinical examination
History taking and physical examination are latecomers to evidence-based medicine. There are intensive efforts in all areas of medicine to base practice on evidence of benefit.
By their nature, physical signs tend to be subjective and one examiner will not always agree with another. For example, the loudness of a murmur or the presence or absence of finger nail changes may be controversial. There are often different accepted methods of assessing the presence or absence of a sign, and experienced clinicians may disagree about whether, for example, the apex beat is in the normal position or not. Even apparently objective measurements such as blood pressure can vary depending on whether Korotkov sound IV or V (page 67) is used, and from minute to minute for the same patient. Some physical signs are present only intermittently; the pericardial rub may disappear before students can be found in the games room to come and listen to it.
Many of the studies that have examined the reliability of physical signs have had problematic variations in disease severity and examiners’ experience.13 This is likely to have led to an underestimation of the reliability of signs.
One way of looking at the usefulness of a sign or a test is to measure or estimate its specificity and sensitivity:
• The specificity of a sign is the proportion of people without the disease who do not have the sign (‘negative in health’). For example, an 80% specificity means that 8 out of 10 people without that sign do not have the condition.
• The sensitivity of a sign is the proportion of people with the disease who have the sign—that is, those who are correctly identified by the test (‘positive in disease’). A sensitivity of 80% means that assessment of the presence of that sign will pick up 80% of people with the condition (but will not pick up 20%).
You may find it helpful to use the following mnemonics to help you remember this:
SpIn = Specific tests when positive help to rule In disease.
SnOut = Sensitive tests when negative help to rule Out disease.
The perfect test or sign (if there were such a thing) is 100% sensitive and specific. A sign or test that is present or ‘positive’ in a person who does not have the condition is called a false positive. The absence of a sign, or a negative test, in a patient who has the condition is called a false negative. Another way of looking at this is the positive or negative predictive value of a test—that is, the probability that a positive result means the condition is present or that a negative result means it is absent. Table 3.4 lists the sensitivity and specificity of some common signs.
TABLE 3.4
Examples of sensitivities and specificities for common clinical signs
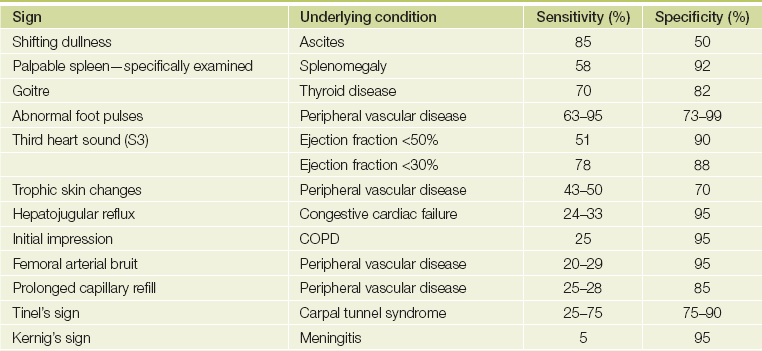
(Anthony MJ, Celermajer DS, Stockler MR. Beauty is in the eye of the beholder: reaching agreement about physical signs and their value. Internal Med J 2005; 35(3):178-187 with permission.)
The likelihood that a test or sign result will be a true positive or negative depends on the prevalence of the disease in the practice setting (or alternatively, what is called the pre-test probability of the condition). For example, if splinter haemorrhages (page 61) are found in the nails of a well manual labourer they are likely to represent a false positive sign of infective endocarditis. This sign is not very sensitive or specific and in this case the pre-test probability of the condition is low. If splinters are found in a sick patient with known valvular heart disease and a new murmur, the sign is likely to be a true positive in this patient with a high pre-test probability of endocarditis. This pre-test probability analysis of the false and true positive rate is based on Bayes’ theorem.
A useful way to summarise sensitivity and specificity is the likelihood ratio (LR). A positive LR indicates that the presence of a sign is likely to occur that much more often in an individual with the disease than in one without it. The higher the positive LR, the more useful is a positive sign. A negative likelihood ratio increases the likelihood that the disease is absent if the sign is not present.


Remember that if the LR is greater than 1, there is an increased probability of disease; if the LR is less than 1, there is a decreased probability of disease. For example, the presence of a third heart sound in a patient who might have heart failure (e.g. breathlessness on exertion) has a positive LR of 3.8 and a negative LR around 1. This means that a third heart sound is specific for heart failure (increases likelihood of the condition nearly four times) but not sensitive (the absence of a third heart sound does not reduce the likelihood).
All these figures are calculated on a population suspected of disease; it would be quite incorrect to apply them to an asymptomatic group of people. Fagan’s nomogram (see Figure 3.13) can be used to apply LRs to clinical problems if the pre-test probability of the condition is known or can be estimated. Remember, positive LRs of 2, 5 and 10 increase the probability of disease by 15%, 30% and 45%, respectively. Similarly, negative LRs of 0.5, 0.2 and 0.1 decrease the probability of disease by 15%, 30% and 45%, respectively.
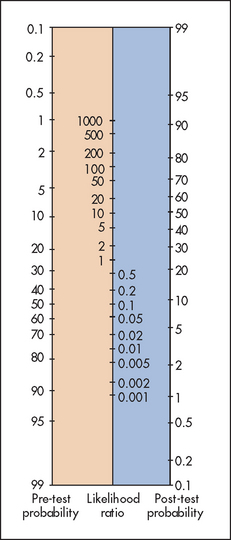
Figure 3.13 Fagan’s nomogram for interpreting a diagnostic test result (Adapted from Sackett DL, Richardson WS, Rosenberg W, Haynes RB. Evidence-based medicine: how to practice and teach EBM. London: Churchill-Livingstone, 1997.) Churchill-Livingstone
When the pre-test probability is very low, even a high positive LR does not make the disease very likely. A line is drawn from the pre-test probability number through the known LR and ends up on the post-test probability number. For example, if the pre-test probability of the condition is low, say 10 (10%) and a sign is present that has an LR of 2, the post-test probability of the condition being present is only about 20%. We have included example LRs in the good signs guides in many chapters of this book.
INTER-OBSERVER AGREEMENT (RELIABILITY) AND THE κ-STATISTIC
The LR of a sign assumes that the sign is present, but there is considerable variability in the agreement between observers about the presence of many signs. There are a number of reasons for this low reliability (see List 3.7).
The κ (kappa) statistic is a way of expressing the inter-observer variation for a sign or test. Values are between 0 and 1, where 0 means agreement about the sign is the same as it would be by chance and 1 means complete (100%) agreement. Occasionally values of less than 0 are obtained when inter-observer agreement is worse than should occur by chance. By convention, a κ-value of 0.8 to 1 means almost or perfect agreement, 0.6 to 0.8 substantial agreement, 0.4 to 0.6 good agreement, 0.2 to 0.4 fair agreement and 0 to 0.2 slight agreement. A selection of signs and their κ-values is listed in Table 3.5. Remember that a high κ-value means agreement about the presence of a sign, not that the sign necessarily has a high positive LR. A low κ-value may be an indication that the sign is a difficult one to elicit accurately, especially for beginners, but it does not always mean that the sign is not useful. For example the detection of the typical fine crackles of interstitial lung disease may have a high κ-value when performed by a group of experienced chest doctors but a low value when assessed by a group of orthopaedic surgeons.
TABLE 3.5
Comparisons of kappa values for common clinical signs (agreement between observers beyond that expected by chance alone)
| Sign | Reliability | Kappa value |
| Abnormality of extra-ocular movements | Substantial | 0.77 |
| Size of goitre by examination | Substantial | 0.74 |
| Forced expiratory time | Substantial | 0.70 |
| Presence of wheezes | Substantial | 0.69 |
| Signs of liver disease e.g. jaundice, Dupuytren’s contracture, spider naevi | Substantial | 0.65 |
| Palpation of the posterior tibial pulse | Good | 0.6 |
| Dullness to percussion | Good | 0.52 |
| Tender liver edge | Good | 0.49 |
| Clubbing | Fair to almost perfect | 0.39-0.90 |
| Bronchial breath sounds | Fair | 0.32 |
| Hearing a systolic murmur | Fair to substantial | 0.3-0.48 |
| Tachypnoea | Fair | 0.25 |
| Clinical breast examination for cancer | Fair to substantial | 0.22-0.59 |
| Neck stiffness | Unreliable | −0.01 |
(Anthony MJ, Celermajer DS, Stockier MR. Beauty is in the eye of the beholder: reaching agreement about physical signs and their value. Internal Med J 2005; 35(3):178-187 with permission.)
Although some of these values appear low, κ-values for the reporting of a number of diagnostic tests have also been calculated and are not much more impressive—for example, the reporting of cardiomegaly on a chest X-ray is 0.48, while cholestasis reported on a liver biopsy is 0.40.
In medical practice, multiple factors are taken into account when diagnostic decisions are made. Only very rarely is one symptom, sign or test diagnostic of a condition. The evidence supporting the usefulness of most signs is based on looking at a sign in isolation. It is much more difficult to study the combined importance of the range of historical and physical findings that are present. However, the skilled and experienced clinician uses many pieces of information and is sceptical when an unexpected or illogical finding or test result is obtained.
Introduction to the OSCE
In most medical schools today, history taking and physical examination are examined using the OSCE (although long and short case testing may also be used). This comprises a series of stations (e.g. 10 minutes each) where particular history or physical examination skills are tested in front of one or two examiners. Students rotate through all of the stations and each station has different examiners. At each station, after a stem or introduction has been provided (e.g. patient’s name, age and presenting symptom), the task to be completed is highly specific (e.g. ‘Please take the blood pressure’). The questions are standardised and pre-set, and the scoring is predetermined, as is (usually) the pass mark. You gain a mark for each necessary step properly completed (e.g. introducing yourself: 1 mark; washing your hands: 1 mark). This means that you must have a system for examination in the OSCE setting and practise it until it becomes second nature.
At the end of most chapters a list of sample OSCE cases and questions is provided to help with revision and as a preparation guide. Look up the answers in the chapter and use this as a way of revising.
At OSCE stations candidates may be asked to take a specific history (e.g. the social history) or examine a particular body system or part (e.g. the praecordium for heart murmurs or the posterior chest for lung signs). Other stations, depending on the students’ seniority, may test clinical skills like prescription writing. Each medical school conducts these exams slightly differently, but there are certain general principles all students should understand (if they wish to pass).
Remember, the ‘patient’ in the exam may be an actor trained to answer questions in a certain way. Actors are also used for the physical examination to test that students complete their techniques properly. The idea of using trained actors is that answers to student questions will be standardised. The actor patients often come from local theatrical schools and there is a risk (albeit tiny) that they will be tempted to overact (e.g. bursting into tears when asked their age; see Figure 3.14). The good news is that all candidates will experience the same conditions.
There are a number of key points to keep in mind during this ordeal:
1. The examiners know how difficult it is to perform while being watched.
2. Their expectations are much lower for students in their first few years of the course.
3. They will give you a spoken or written introduction, or both. This will tell you what they expect you to do, so don’t do something different. For example, if the request is to examine the upper limbs of a patient with weakness in the arms, don’t begin by testing sensation. Time is limited and the examiners will have directed you to where the abnormal signs will be (if there are any, which often there are not in this type of exam).
4. As important to the examiners as a good technical approach is your attitude to the patient. You can expect to fail if you are rude and inconsiderate.
5. It is important to develop a routine when you practise for these exams. This includes introducing yourself and explaining at the start, and then with each step, what you are going to do. For example, if asked to examine the patient’s abdomen, having introduced yourself, say something like ‘I have been asked to examine your abdomen. I will need you to lie flat for me with just one pillow. Will you be comfortable like that? I will need to pull your underpants down a little lower. Is that all right? Are you sore anywhere? I’m sorry my hands are a little cold. Please let me know if this is at all uncomfortable for you.’ Make it clear during the examination that you are watching the patient’s face for any sign that the examination is painful. This type of approach to patients is really only normal politeness and should be routine (i.e. not just used during exams).
6. Remember to wash your hands before and after for an easy mark (and in practice you should always do this to protect the patient and you).
A video-recorded OSCE examination is provided with this edition to help guide you further. There is more help online; for example, search for Wikiversity’s OSCE review or Instamedic. There are also useful phone apps available.
References
1. Sacket, DL. The science of the art of clinical examination. JAMA. 1992; 267:2650–2652. [This article examines the limitations of current research in the field of clinical examination.].
2. Sackett, DL. A primer on the precision and accuracy of the clinical examination (the rational clinical examination). JAMA. 1992; 267:2638–2644. [An important article examining the relevance of understanding both precision (reproducibility among various examiners) and accuracy (determining the truth) in clinical examination.].
3. Wiener, S, Nathanson, M. Physical examination: frequently observed errors. JAMA. 1976; 236:852–855. [This article categorises errors, including poor skills, underreporting and overreporting of signs, use of inadequate equipment and inadequate recording.].
4. Fitzgerald, FT, Tierney, LM, Jr. The bedside Sherlock Holmes. West J Med. 1982; 137:169–175. [Here deductive reasoning is discussed as a tool in clinical diagnosis.].
5. Sackett, DL, Haynes, RB, Tugwell, PClinical epidemiology. A basic science for clinical medicine. Boston: Little, Brown & Co, 1985. [The perceived commonness of diseases affects our approach to their diagnosis.].
6. Cretikos, MA, Bellomo, R, Hillman, K, Chen, J, Finfer, S, Flabouris, A. Respiratory rate: the neglected vital sign. Med J Aust. 2008; 188(11):657–659.
7. Martin, L, Khalil, H. How much reduced hemoglobin is necessary to generate central cyanosis. Chest. 1990; 97:182–185. [This useful article explains the chemistry of haemoglobin and its colour change.].
8. Detsky, AS, Smalley, PS, Chang, J. Is this patient malnourished. JAMA. 1994; 271:54–58. [Assessment of nutrition is an important part of the examination but needs a scientific approach.].
9. Gross, CR, Lindquist, RD, Woolley, AC, et al. Clinical indicators of dehydration severity in elderly patients. J Emerg Med. 1992; 10:267–274. [This important and urgent assessment is more difficult in elderly sick patients.].
10. Koziol-McLain, J, Lowenstein, SR, Fuller, B. Orthostatic vital signs in emergency medicine department patients. Ann Emerg Med. 1991; 20:606–610. [These signs help in the assessment of the severity of illness in emergency patients, but there is a wide range of normal.].
11. McGee, S, Abernethy, WB, III., Simel, DL. Is this patient hypovolemic. JAMA. 1999; 281:1022–1029. [The most sensitive clinical features for large-volume blood loss are severe postural dizziness and a postural rise in pulse rate of >30 beats per minute, not tachycardia or supine hypotension. A dry axilla supports dehydration. Moist mucous membranes and a tongue without furrows make hypovolaemia unlikely; assessing skin turgor, surprisingly, is not of proven value.].
12. Hayden, GF. Olfactory diagnosis in medicine. Postgrad Med. 1980; 67:110–115. [118. Describes characteristic patient odours and their connections with disease, although the diagnostic accuracy is uncertain.].
13. Benbassat, J, Baumal, R. Narrative review: should teaching of the respiratory physical examination be restricted only to signs with proven reliability and validity. J Gen Intern Med. 2010; 25(8):865–872. [Physical signs in respiratory disease generally have lower than ideal reliability and sensitivity, but some signs have high specificity. While physical examination of the chest should not be ignored, more research is needed!].