Chapter 8 The human lifespan and its effect on selecting nursing interventions
Introduction
This chapter aims to provide an overview of the multifaceted process of development that occurs throughout a person’s life. It begins with an outline of two social sciences, psychology and sociology, with explanation of contrasting approaches to both, which recur throughout. Key topics from each subject are explored, namely motivation, culture, socialization and family. Physical development is described from conception through infancy and childhood milestones, adolescence and adulthood to old age. Psychosocial development covers the emergence of the self-concept, cognition and morality, emotional attachment and separation, aspects of sexuality and personality, and social integration. Implications of this subject matter for student nurses and nursing practice are highlighted as they arise, i.e. why it is important for all nurses to be aware of patients’ developmental issues when planning and implementing their care.
Psychology and sociology related to development and nursing
This section outlines the psychological and sociological theories, approaches, frameworks and important topics such as motivation and culture required for understanding developmental processes.
What is psychology?
Gross (2001) has described how psychologists seem to provoke three typical reactions in others. These are:
The word psychology is a composite of the Greek term psyche, which refers to the ancient view of the soul, spirit or mind, and logos, which means discourse or intellectual debate, a then-favoured method of pursuing investigation or study. Thus, in modern terms, it can be taken to mean ‘the study of the mind’, or of mental processes, and it is clearly useful for nurses to understand what is going on in a patient’s/client’s mind and the resulting consequences, i.e. patient behaviour.
The father of psychology is usually identified as Wilhelm Wundt who, in 1879, initiated scientific research into the mind. Wundt aimed to study perceptual discrimination of sensory input, e.g. vision under controlled conditions, and so develop an understanding of what he termed the ‘elements of consciousness’, building blocks of the mind. He felt able to investigate discernible differences in intensity and quality of stimuli, and so begin to describe the structure of the human mind – termed the ‘structuralist’ approach to psychology.
William James likened Wundt’s method to trying to understand a house by contemplating its individual bricks, and considered that the ‘whole’ mind as an integrated entity was of more significance than the sum of its parts, inspiring the Gestalt viewpoint, which gained currency from the 1920s. James was more interested in what the mind could do and what it is for, i.e. the ‘functionalist’ approach. This focuses on studying thoughts and emotions, and how they help people to survive in their envir-onment. From these early origins, this hybrid discipline branched into at least three distinct schools or approaches – psychodynamic, behaviourist and humanistic.
Psychodynamic approach (see pp. 212, 214 and 218)
This stemmed from the publications of Sigmund Freud from the 1890s onwards. Essentially, this emphasized the importance of unconscious processes in emotions and behaviours. Freud developed a therapeutic approach called ‘psychoanalysis’, designed to gain access to the unconscious mind using means such as hypnosis, tranquillizing medication and dream analysis.
Behaviourist approach
By the early 1900s, American academics such as J.B. Watson had become increasingly critical of the subjective methods used by Freud and Wundt. They argued that mental events were inaccessible to and therefore inappropriate for scientific investigation. It was argued that psychologists should concentrate on dispassionately and accurately observing outward behaviour, for example responses to experimentally controlled stimuli. Much of the behaviourists’ focus was on studies of animal learning, which they viewed as taking two forms:
This approach assumed the validity of comparisons between humans and animals, and that environmental factors can and could be used to determine or ‘shape’ an individual’s behaviour, just as animals can be trained to perform skills beyond their normal repertoire. Psychologists could thus devise methods of engineering people’s behaviour in ‘desirable’ directions by means of ‘conditioning’ programmes. Behaviourism held sway in psychology until after World War 2, when its emphasis on animal observation and scientific rigour began to be questioned.
Humanistic approach
A new school of psychologists, including Abraham Maslow and Carl Rogers, then emerged as a ‘third force’ in this subject. The humanists focused on aspects of purely human experience, such as free will and self-fulfilment. Their methods of enquiry were subjective and person-centred, such as interview and self-report. Offshoots included therapeutic self-help groups and learner-directed educational approaches. Humanism emphasizes the positive potential in people and the importance of fostering appropriate individual choices in maximizing each person’s well-being and life satisfaction.
Applying psychological approaches to health
The three approaches can be exemplified with reference to a health issue such as smoking, as follows.
Motivation
Motivation is the underlying cause of actions. Without it people would be inert and not function. It provides individuals with the stamina and focus required to perform their activities.
Essentially then, motivation is used to explain behaviour. Without apparent explanation, behaviour may appear to be fruitless, perplexing or dangerously unpredictable. Nurses need to understand what happens in their environment, including the actions of others, not only to be able to predict eventualities but also to plan their own behaviour and interventions appropriately. Box 8.1 provides an opportunity to consider the motiv-ation to become a nurse.
 REFLECTIVE PRACTICE
REFLECTIVE PRACTICEMotivation to become a nurse
Think about your reasons for becoming a nurse. It may be useful to compare your reasons with those of colleagues, and note any that are different from your own.
Student activities
The ‘instincts’ theory of motivation
Early psychologists studied animals and compared their behaviour with that of humans, who were viewed as the most evolved and complex members of the animal kingdom.
Consider the question, ‘What makes cats hunt, birds sing and monkeys climb?’ The usual response is their respective ‘instincts’. The next question to address is, ‘What is meant by the term instinct?’ A reasonable answer might be a complex, unlearned behaviour pattern, i.e. more than a single reflex, specific to a species, which is elicited by a specific stimulus or ‘releaser’, e.g. a mouse appearing in front of a cat. The word derives from the Greek to ‘impel’ or ‘instigate’.
‘Acting on instinct’ is often used to describe automatic behaviour, such as using touch to comfort a distressed patient. However, many consider that there are no evident instincts in humans, as it can be argued that even seemingly natural characteristics such as associating with others, sexual desire, masculine aggression, parenting and intuition all involve some process of learning and are not always present.
Early attempts by William McDougall to explain all human behaviour in terms of instincts foundered on two problems. Firstly, because of the complexity and variability of human behaviour, his approach with 800 separate instincts was unconvincing in explaining why humans differ from each other so widely in preferences and responses, as only some humans hunt, sing and climb, and very few enjoy all three. Second, this approach was criticized for its lack of explanatory value, because it led to a circular argument. The question, ‘What makes humans act in certain ways?’ would prompt the answer ‘instincts’. To the follow-up query, ‘What are instincts?’, MacDougall’s response might have been ‘things we naturally possess that make us act in those ways’.
Freud proposed that just two instincts motivated behaviour:
Behaviourist theories of motivation
In the 1950s, Lorenz demonstrated that newly hatched goslings follow the first large moving object, whether either himself or an inanimate figure that they are exposed to in a critical period during their early days of life – thought to be an instinctive releaser normally allowing them to be led to the relative safety of water. Subsequently they were described as behaviourally attached to or ‘imprinted on’ this initial figure as their particular, if experimentally odd, ‘Mother Goose’.
It is possible to suggest examples of critical periods, releasers or imprinting in human development. For instance, there is considerable evidence that language acquisition (see Ch. 9) and ‘healthy’ personality development – socialization (pp. 194–195) and attachment (pp. 212–214) – are dependent on exposure to normal human society in the first 4 years of life. Parental feelings and caring skills may be experienced or ‘released’ for the first time after having one’s own child and, in some cases, following a parent into nursing may be considered to be an example of imprinting.
Drive theory
Clark Hull argued that all behaviour was impelled by ‘drives’, hypothetical internal states arising from ‘needs’. Figure 8.1 shows how this approach can be used to explain increased fluid intake on a hot day, essentially a homeostatic mechanism (Ch. 19).

Hull’s theory explains biological or ‘primary’ needs relating to homeostasis, such as hunger, thirst and sleep, but seems less convincing when proposing ‘secondary’ drives to explain the wider range of human pursuits, e.g. intellectual or social activities.
Nonetheless, the terms ‘drive’ or ‘driven’ are often used conversationally with regard to motivation, and Hull’s framework accords well with the experience that it is sometimes better to want or pursue something than to attain it.
Humanistic approach to motivation
Humanists believe that people are unique in possessing a rich mental life, including free choice of action, dreams and personal goals, rendering behaviourist comparisons with other species futile.
Maslow proposed a ‘hierarchy of needs’ to explain human behaviour. Although this originally comprised five levels of need, two more levels have since been added. Note that some descriptions omit levels 5 and 6 shown in the 7-level adaptation (Box 8.2). The goal at the highest tier of the hierarchy is individual fulfilment or self-actualization, but this can normally only be attained following prior satisfaction of lower levels of need. The hierarchy of needs can be represented as a pyramid with self-actualization at the apex and the physiological needs at its base (see Atkinson et al 2000).
Box 8.2 Maslow’s hierarchy of human needs
3 Love and belongingness (affiliation) needs
Giving and receiving affection; trust and acceptance of others, being part of a group
* Omitted in some descriptions.
Examples of how nurses may help patients/clients to meet needs at each level include:
Maslow’s concept of self-actualization is embodied in peak experiences, cherishable moments of ecstatic happiness when everything seems to ‘gel’ and feels right, and a person’s essential current ambition is fulfilled. He considered that all humans were capable of these, although they are usually infrequent and some may occur ‘once in a lifetime’.
There are, however, exceptions to the hierarchical structure of lower needs always being fulfilled before higher needs. It is possible to identify valid exceptions to Maslow’s order of priorities. For instance:
What is sociology?
Definitions vary, and often reveal the standpoint of the writer. Macrosociology emphasizes the study of society overall, while microsociology focuses on the interactions of individuals within it. All degrees of magnification in between these extremes are possible, for instance when studying groups within society. Health workers can be considered through the one-to-one dealings of individual nurses with their patients/clients, the functioning of ward teams or types/grades of nurses, the profession as a whole, or the entire NHS workforce.
The focus could enlarge further to cover people in Britain, Westerners or, indeed, all mankind. Sociology can therefore be defined as the study of societies, their component groups and individual interactions.
However, all sociologists would agree that people cannot be understood as individuals in a vacuum; to be human is to be social. People arise from social groups and from within society, and are part of its fabric during their lifespan. In effect, people are society, i.e. each person is equivalent to a brick within the building and society is ‘within each person’, as contact with others in society shapes each person. Because of this, nurses can only understand others and themselves by appreciating this social dimension common to all people.
Several sociologists’ views have been particularly influential over the 19th and 20th centuries; an outline is provided in Box 8.3 (see p. 190).
Box 8.3 Influential sociologists
Auguste Comte
During the 19th century the French ‘Father of Sociology’ was positive that his ‘Queen of Sciences’ would establish truths about recently urbanized, ‘industrial’ society and so be able to prescribe remedies for its human difficulties. This gave him the confidence to dub himself the ‘Great Priest of Humanity’ and his optimistic outlook has been shared by many of his successors.
Karl Marx
Marx was particularly conscious of the extreme economic inequalities within newly industrialized mid-19th century society. He predicted that the masses of employed workers – ‘the proletariat’ – would come to realize their exploitation and the need to wrest ownership of factories and land, the source of societal wealth, from their employers, the capitalist minority. The post-revolutionary sharing of society’s ‘means of production’ would inaugurate an era of classless, socialist utopia.
Max Weber
Weber modified Marx’s economic ‘conflict’ interpretation of society by focusing more narrowly and deeply on the perspectives and interactions of individuals and groups within society. For example, he noted the diversity of skills, status and aspirations within the working class, which Marx had tended to treat as a homogeneous mass. Weber also emphasized the usefulness of greater subjectivity within sociology, empathy being a prerequisite to understanding the shared meanings in human interactions – verstehen. An example of this approach would be to consider the many possible factors contributing to the anxiety experienced by a patient newly admitted to hospital.
Emile Durkheim
Comparative study between societies was Durkheim’s hallmark. He used newly accumulated data on populations, such as census information, to make deductions about the actions, thoughts and feelings of individuals. In particular he came to view suicide as a reflection of the circumstances, expectations and laws of the groups, organizations and society to which one belongs, rather than a purely private, individual act. It is only possible to understand phenomena such as ‘suicide bombings’ by taking their social context into account.
Park, Cooley and Mead
In the United States, the 19th and early 20th centuries saw huge expansion of industrial cities, which together with mass immigration led to many social problems such as crime, ghetto squalor and intergroup hostility. Robert Park and his colleagues used the city of Chicago as a laboratory for research ‘in the field’, while Charles Cooley and G.H. Mead worked on the social interactions of key significance in childhood development (see the ‘self’, pp. 204–207).
Talcott Parsons
During the 20th century Parsons formulated a comprehensive theory of society as a functioning entity, with each individual, group and organization playing its part or ‘role’ to make the system work and deriving benefits in return for their contribution. This represents an alternative macrosociological (‘big picture’) structuralist perspective or viewpoint to that of Marx on societal study, looking at society as a single, whole entity. Parson’s ‘structural functionalist’ or ‘consensus’ approach views society as a harmonious arrangement wherein people basically agree on fundamental operational principles. This enables society to operate or function effectively. Each member works to benefit society, and in return active membership benefits each member, e.g. nurses provide health care, while potential patients transport them to work or provide food for them.
Conflict approaches
These consider society as characterized by competition between antagonistic groups, each in pursuit of opposing interests. These include:
Conflict perspectives characteristically argue the need for radical revision or overthrow of society’s attitudes, institutions and general way of life.
Microsociological approach
This focuses on the individuals and groups whose daily interactions comprise society’s life, e.g. how nurses behave towards patients/clients and their colleagues, the experiences of student nurses in clinical areas or whether nursing is a ‘profession’. Such studies view people as entering social situations with pre-existing ideas about themselves, others and the situation, e.g. their relative status and expected actions, and this subjective perspective largely determines their interpersonal behaviour. Members of a society possess shared meanings in the use of symbols such as language, gestures and other non-verbal behaviour including dress, focus on which is often termed ‘symbolic interactionism’ (see Ch. 9).
Why is sociology relevant to nursing?
Consider the following quotation:
No man is an island, entire of itself … any man’s death diminishes me because I am involved in mankind; and therefore never send to know for whom the bell tolls, it tolls for thee.
The excerpt from this 17th century poet’s meditation compares a man’s death to a clod of earth being washed into the sea. It emphasizes how inextricably each person is bound up with other members of their society and its groups, even if the person is not conscious of this communality in their individual day-to-day pursuits and concerns. It is reminiscent of the sociobiological explanation of why people are inclined to help others – the cardinal function of nursing. Due to a common evolutionary ancestry, this argues that all humans are genetically related to each other, so that assisting others to survive helps preserve some of their own genes.
Knowledge of sociology helps nurses to understand the behaviours of patients/clients, families and colleagues. For example, a patient’s/client’s outward distress is automatically attributed to physical pain, or else fear regarding the experience or findings of an operation (Box 8.4). In other words, physical or psychological factors specific to the individual tend to be the initial assumption.
 CRITICAL THINKING
CRITICAL THINKINGMichael
Michael is recovering from surgery, which has been technically successful. Despite having received appropriate information and nursing care to maximize his physical comfort, he remains restless, tearful and frequently demands nursing attention.
However, patients’/clients’ concerns often arise from a wider social context, such as worries about family members, employment or even care of pets. A patient/client might be more concerned about being forbidden to move heavy items at work after back surgery and the effects on their livelihood and self-worth than about any transient postoperative pain or discomfort. Health professionals rarely gain such insights from case notes or superficial encounters with the patient/client; they often emerge only when imparted in the context of a trusting relationship with the patient/client, which takes time and effort to develop (see Ch. 9).
Sociology provides insights into aspects of the nurse’s own culture and, by logical extension, into different cultures, particularly significant with the increasing cultural diversity of British society. Examples of this include the social practices specific to some members of minor-ity groups. A patient/client or their relatives may be upset or feel offended if an otherwise caring environment fails to accommodate their cultural norms such as food preferences, consultation of their spouse or prayer requirements.
This awareness can also be turned to enhancing the nurse’s self-understanding, for instance by analysis of their own social experience (Box 8.5).
Adjusting to new nursing environments
All student nurses encounter unfamiliar settings at the beginning of new placements, which can provoke anxiety.
The layout, titles and respective roles of new colleagues, in addition to the names and needs of the current patients/clients, must all be learned. The management style of the charge nurse on any day may be important, for example whether the use of first name terms is mutually acceptable and how strict time constraints are for completing tasks or meal breaks. Appropriate use of initiative has to be gauged through experience, and may be quite different for a nurse in a student role compared with their concurrent part-time or former auxiliary role, perhaps in the same environment. Understanding the dynamics of this process may help to diminish the stress of the new placement.
Sociology can also shed light on larger scale social issues, possible remedial strategies and insight into the effectiveness of these measures, e.g. by performing research and analyzing its findings (see Ch. 5). Approaches include compiling and analysing quantitative data, e.g. the incidence of teenage pregnancy, and qualitative measures such as surveying attitudes, e.g. to binge drinking or unprotected sex.
Whatever their focus and theoretical standpoint, it would be hoped that social scientists would provide insightful appraisal of social realities to at least complement those offered by religions and secular common sense.
Common sense and sociology
Nurses need to consider how sociology can enhance commonsense thinking (Box 8.6). Further discussion of sociology and commonsense is available in Further reading (e.g. Giddens 1989).
Is commonsense all we need?
Read the statements below and decide whether they are true or false.
Perhaps the best way to ensure a long life is to pick healthy parents, as longevity or brevity tends to run in families. However, although genes play a role in determining susceptibility to many diseases, environmental factors appear to contribute equally as significantly. This explains the close association between health and wealth, apparent in the significantly raised incidence of nearly all serious disease categories among the poorest sections of society (Townsend & Whitehead 1990) (see Ch. 1). Relevant factors include quality of housing, diet, occupation, leisure activities and, more controversially, healthcare provision. Thus a person’s family environment may have much more significance to health than their genes.
Regarding the second statement, most older adults retain their mental vigour with only around 5% of those over 65, and 20% of those over 80 years of age, exhibiting dementia (Alzheimer’s Society 2006). They undoubtedly represent stores of accumulated knowledge and skills, distilled into wisdom by a lifetime’s reflection on their experience. Despite this, older adults in Western society have been typically viewed as a redundant group who are an economic burden on the productive section of society. They tend to be functionally marginalized, i.e. excluded from the social mainstream in, for example, occupation and leisure, rationed in resources such as facilities and benefits, and viewed not with respect but in a derogatory manner, ranging from well-meaning pity to outright contempt, some of the many expressions of ageism.
Although education is often regarded as the key to universal achievement and equality, there is much to suggest that the Western system tends to perpetuate and cement inequalities. Middle-class children tend to achieve more and better qualifications than their working class counterparts, perhaps in part because their parents provide better preparation, encouragement and facilities, but also because they seem to relate more easily to teachers and their style of communication. This disparity is accentuated by other social factors that predominate in the working class such as early pressure to earn, widely varying facilities even within the state system and peer group behaviours. Thus children from affluent backgrounds are more likely to progress directly to full-time higher education and from there to better paid jobs, often in their parents’ professions.
Culture
Take a moment to think of what the term ‘culture’ means to you. Common responses include normal patterns of behaviour within one’s country, including eating, drinking and speech, and ‘lofty’ forms of social expression such as art, music and literature.
Culture can be defined as the way of life of a society – a group of people who share a distinct identity, often within a circumscribed locality. Components of a culture include beliefs, values and norms.
It is, however, important to remember that the components of culture typically change within a society over time, allowing it to gradually adapt to changing circumstances and evolve. An example of this is the insistence in the late 19th and early 20th century that student or ‘probationer’ nurses were all female and would attend Christian services each Sunday, stay within the nurses’ home when not on duty and leave the profession once married (see Ch. 2). This is quite different to experiences of student nurses in the 21st century.
Beliefs
These are factual ideas such as religious beliefs about whether there is one God, or more, or none. Some beliefs may involve lifestyle issues, e.g. a nutritional belief about what is good or bad to eat, or how it should be prepared, which varies hugely between societies, as does the acceptability of alcohol. Traditional cultures may revere people who see visions and hear divine voices, whereas in Western cultures a psychiatrist is likely to be consulted.
Values
These are broad guidelines for activities, conveying what principles a society deems valuable or worth preserving. In the West, freedom of speech, occupation and choice of partner is highly prized, which may conflict with values such as patriotism, equality of wealth and respect for older people, which are more esteemed in other soci-eties. Values tend to be more absolute than beliefs, i.e. are subscribed to whole-heartedly or not at all, so that optimizing ‘health’ may either govern one’s lifestyle fully or not at all. The sanctity of life, i.e. that life is precious and should not be taken intentionally, is another value central to healthcare but not to all human situations.
Norms
These are more specific behavioural expectations rele-vant to particular circumstances, equivalent to everyday ‘do’s’ and ‘don’ts’. For instance, personal greetings such as tongue protrusion are expected in Maori ceremonies but not at social gatherings in the Western world, there are occasions where polite versus familiar speech is expected, eating etiquette including table manners and fashionable attire. Conformity increases the likelihood of social acceptance and success, e.g. belching is rarely appreciated at formal dinners in the UK, and often mirrors the underpinning value, e.g. paying for goods reflects honesty or adhering to nursing advice suggests that a patient/client values health. Norms are in turn often subdivided into folkways, customs, mores and rules (Box 8.7).
Cultural universals
As well as the foregoing components, some elements of culture are common to all societies. For example language, both verbal and non-verbal, enables interpersonal communication (see Ch. 9). Mutual understanding of the spoken and written word can give members of a society a unique communal currency, especially if fluency is restricted to small populations, e.g. the Celtic tongues in the UK.
Facial expressions conveying universal emotions such as joy, sorrow, fear and surprise are recognized across cultural groups, but conventions governing the meaning of gestures and acceptable degrees of interpersonal touch and distance vary widely. Other aspects probably common to all cultures, past and present, include:
Cultural bias and relativism
Comparing the different practices and underpinning belief systems of different cultures tends to encourage people to favour those of their own society. There are many possible reasons for this bias. These include respect for those people who have nurtured them, greater famil-iarity with their own ways and boosting group self-esteem through criticizing foreign behaviours. However, in a culturally diverse society, this may lead to intergroup hostility and discrimination, resulting in unequal treatment, not least in healthcare settings. Thus it is important to remain aware of this tendency, and to try to accept these differences as indicators of the distinctiveness of a particular group rather considering whether they are better or worse than one’s own experiences. Aspects of Western culture, which might strike an outsider as different or unusual, are considered in Box 8.8.
Subcultures
Individuals within a society form groups that have their own distinctive views and practices. These variations inside a culture give rise to subcultures – effectively ‘cultures within a culture’. A common example is youth culture, as young people have typical values, beliefs and norms such as a code of conduct in relation to dress, speech and musical taste. These may vary markedly from those of older adults who comprise the influential majority and so the cultural yardstick of society. Other ‘variant’ subcultures include those of minority ethnic groups, students and healthcare professionals. Some subcultures overtly refuse to comply with existing laws in a society, and are termed ‘deviant’ subcultures, such as criminal gangs. ‘Counter-cultures’ are antagonistic towards the prevailing dominant culture, although they may not break any of its legal statutes, e.g. travelling people, self-sufficient smallholders and pacifist campaigners in the UK (Giddens 2001).
Culture shock
This is the term given to the sense of disorientation experienced when exposed to an unaccustomed culture or subculture. Varying degrees of this occur when on holiday abroad, when entering a new workplace or setting (Box 8.9). Admission to hospital or to a care home may provoke anxiety. The possible stressors (see Ch. 11) associated with the hospital/care home subculture might include:
Culture shock
Think about a time when you became part of a new subculture, for example starting a new school, meeting your partner’s family or starting your nursing course.
Student activities
Culture and healthcare (see Ch. 1)
A profound interconnection exists between these two. People from different cultures may have conflicting ideas about what constitutes health or illness, for example the diagnostic criteria for mental health problems such as schizophrenia differ enormously between Western and Eastern perspectives, and studies have shown wide cultural variations regarding pain tolerance (see Ch. 23), risk-taking behaviours, e.g. use of cannabis by Rastafarians, and unsafe sexual behaviours and the spread of the human immunodeficiency virus (HIV) in sub-Saharan Africa.
Nurses have to be sensitive to the cultural expectations of individual patients/clients and families, without making stereotypical assumptions, if they are to deliver holistic care (Box 8.10). This may involve aspects that include:
Cultural awareness in nursing practice
You are helping the registered nurse (RN) to admit a client who is anxious about being admitted to the unit. The RN asks the client for his Christian name and is surprised when he challenges her by saying that he is Muslim.
Student activities
[Resource: BBC (Religion and Ethics) – www.bbc.co.uk/worldservice/people/features/world_religions/index.shtml Available July 2006]
Socialization
This is the process whereby a society transmits its culture (or group its subculture) to its future members. As a result, individuals acquire the knowledge and skills that allow them to function socially, leading to personal and communal success. Socialization is usually described in two phases: primary and secondary (Box 8.11).
Personal experience of socialization
Think back to an episode when you learned something from a parent or person close to you, from the mass media and from a RN while on placement.
Student activities
Note: You may find that feelings significantly colour such recollections. As socialization is an interpersonal process, it often imparts learning in a profound and emotional manner.
Socialization is a two-way process throughout, with the novice challenging the ‘mentor’ by asking questions and proposing alternatives, so that becoming a parent involves learning from interactions with one’s children, and the same give-and-take occurs during grandparenting.
Primary socialization
This occurs in early childhood, and the main ‘agents’ are usually close family members. The preschool child acquires fundamental skills relating to interaction with others including speech, gesture and appropriate behaviour, and self-care, e.g. continence, dressing, feeding. In addition, attitudes including moral and religious beliefs are transmitted. On occasions, teaching can be formal, or deliberate, such as instruction on tying shoelaces. At other times, it may be imparted unconsciously, or informally, as when a child overhears their parent’s private opinion about something. Because of the initial and personal nature of this process, primary socialization often carries profound emotional undertones, and may cement lifelong memories and bonds.
Secondary socialization
This refers to cultural transmission that occurs from entering school, and continues throughout life. It equips the growing person to survive and prosper outwith the family environment; its agents include teachers, peers (equals such as friends and fellow students), work supervisors and colleagues, and the mass media, e.g. authors, journalists and broadcasters.
The term tertiary or ‘professional’ socialization (see p. 207) is sometimes used in relation to the acquisition of knowledge, skills and attitudes required in performing high-level occupations such as nursing.
Roles
Functionalist sociology pictures socialization as gearing individuals to fulfil roles, which are social positions involving expected behaviours. Each person typically performs several roles, usually focusing on one at a time, including some that are:
It can be seen that many roles have reciprocal partners, in that one to some extent defines the other, so that it is hard to imagine the traditional role of nurse or doctor without someone filling the role of patient/client.
Each role can be viewed as beneficial to other members of society but also to the performer; although every role has its duties or obligations, it also confers rights and privileges if carried out adequately (Box 8.12).
Thus society can be viewed as a symbiotic community, each role-bearer contributing to its smooth running, and in turn receiving rewards such as healthcare when sick. Parsons extended this framework to formulate the ‘sick role’, which people could legitimately adopt when ill, as in such circumstances they could not fully perform their normal roles (see Ch. 1). As with all roles, this conferred rights and privileges, provided the sick person fulfilled certain duties and obligations.
Role conflict
Fulfilling several roles can be a tricky balancing act and sometimes ‘role conflict’ is inevitable. It occurs where the demands of fulfilling one role impairs the performance of another, such as family commitments undermining focus on study or nursing duties (Box 8.13, p. 196).
Potential role conflict
Student Nurse Sarah has two children of school age. Her husband is in full-time employment, and Sarah works as a care assistant two days a week to supplement the family income.
Often domestic commitments detract from energy and available time for family relationships, study and other work. Caring for dependent older relatives can also have a significant impact on a person’s own parenting, work and personal life.
The family
A person’s understanding of the term ‘family’ pervades the way in which they view the world. This is evident in the use of terms such as ‘Father Time’ and ‘Mother Earth’. Political parties vie to be the ‘party of the family’ and espouse ‘family values’, and the family is often regarded as the basic unit, or even a microcosm of society (Box 8.14).
What ‘family’ means
Although a term used in everyday speech, it is not easy to agree on a universally acceptable or concise definition of ‘family’.
The term ‘family’ means different things to different people, but the common associations it raises are emotions such as love and affection, or possibly mixed or negative ones, personal closeness, intimacy and shared experiences, communal housing, financial support, advice, the roles mentioned earlier and caring for one another.
Although people can have different family experiences, a general definition is ‘a group of people, bound by kinship ties, who live together, share resources and who look after each other in times of need’. All societies have some form of family unit that performs – although some would say controls – essential functions including the reproduction, economics and socialization of its members.
Family structures
Family structures vary widely both between and within cultures. Common variants include:
In addition to its universality and pivotal position in society, the family has received much consideration as either an integral part of healthcare provision or a contributing factor to many physical and mental health problems.
There are many ways in which the family may be significant for an individual’s health and healthcare, both positively and negatively. These include transmitting ‘healthy genes’ or those producing abnormal conditions; providing the emotional climate surrounding child-rearing and adult interactions, e.g. loving care or forms of abuse. Communication patterns may be supportive or disruptive to mental health, and family income is usually crucial in determining material comfort. Links between wealth and health are well documented (Ch. 1); lifestyle choices such as diet, smoking and exercise are often influenced by domestic attitudes. Close relatives may be understanding of, or intolerant of, certain conditions, e.g. learning disabilities, mental health problems, substance misuse or HIV infection. Family dynamics may involve either mutual devotion to or guilt at not shouldering the burden of a family member’s care needs. Relatives may also disagree with care decisions, e.g. prolonging active treatment or disclosing poor prognosis, and place great value on customs required for a loved one’s care or treatment (Denny & Earle 2005).
As with individuals and the culture in which they exist, the family does not remain static but continuously evolves to adapt to changing pressures and circumstances. In many ways it represents a mirror of society at any given time, reflecting its development, limitations and current challenges, its successes and its shortcomings.
Trends in family structures
Considerable changes in family structure have taken place over the last few decades.
Some examples of these trends, as suggested by Abercrombie and Warde (2005), and which do not necessarily apply to all social groups or countries, include the following:
Development across the lifespan
As late as Victorian times, children were viewed as small adults, pre-programmed for adult knowledge and behaviour to emerge with passing years. This view, which implies the importance of natural growth in physical size and strength, changed with greater awareness of child exploitation and misery, e.g. in the novels of Charles Dickens. Protective legislation began to confer rights on children, such as education. Prior to 1833, under nines could work up to 12 hours a day in factories. Only after the Education Act of 1870 did attendance at school become compulsory for most children until age 13 in the UK; the leaving age became 15 only after World War 2 and 16 years in 1972. Another factor in reappraising childhood was the increasing scientific interest in the process of adaptation that followed Darwin’s publications on evolution. From the early 1900s, much enquiry focused on how the individual’s concept of ‘self’ was formed, parallel with Freud’s contemporary ideas on unconscious processes being formative in adult sexual and personality patterns. The latter was to inspire Erikson’s model of a person integrating socially through their resolution of a series of ‘personal crises’. The middle part of the 20th century saw much investigation of how cognitive, moral and emotional maturity is acquired, such as through the work of Piaget, Kohlberg and Bowlby.
This section outlines the important stages of physical and psychosocial development throughout the lifespan. Factors affecting development and their potential signi-ficance to health are briefly considered. Developmental milestones from birth to school age are introduced, and the Denver II (1990), a developmental screening test (previously known as the DDST), is included (pp. 202–203). Detailed discussion of the developmental milestones is beyond the scope of this book and readers requiring more information should consult Further reading (e.g. Hockenberry et al 2002).
Physical development
This section outlines how the body grows and develops before birth and then through the stages commonly identified thereafter, namely infancy, childhood, adolescence, adulthood, middle and old age. Chapter 14 provides further information about monitoring children’s growth in height and weight gain.
Various hormones influence growth and development throughout the lifespan, such as those that stimulate growth during infancy and those that initiate the events of puberty. Some examples are outlined in Table 8.1 (see p. 198).
Table 8.1 Hormones affecting growth and development (after Hinchliff et al 1996)
| Hormone | Source | Effects |
|---|---|---|
| Growth hormone (GH) | Anterior pituitary gland | Stimulates growth in many tissues, e.g. bone and skeletal muscle |
| Stimulates protein synthesis | ||
| Cell growth and repair | ||
| Thyroid hormones | Thyroid gland | Needed for normal development of central nervous system |
| Deficiency during early childhood results in small stature and impaired mental development and learning disability | ||
| Parathyroid hormone with vitamin D and the hormone calcitonin secreted by the thyroid gland | Parathyroid glands | Bone growth and formation |
| Insulin | Pancreas | Glucose uptake |
| Inhibits protein breakdown and stimulates protein synthesis | ||
| Glucagon | Pancreas | Glucose usage |
| Rapid rise in blood glucose level | ||
| Glucocorticoids, e.g. cortisol (see also Ch. 11) | Adrenal glands (cortex) | Regulates tissue growth |
| Excess during periods of growth inhibits growth in height | ||
| Oestrogen | Ovaries | Female secondary sexual characteristics |
| Female body fat distribution | ||
| Bone density | ||
| Testosterone | Testes | Male secondary sexual characteristics |
| Widespread anabolic effects on many body (somatic) tissues to produce male physique |
Conception to birth
Almost every month following the establishment of menstrual cycles during puberty until the menopause (cessation of menstrual cycles), a non-pregnant woman ovulates or releases usually a single oocyte, or egg, from one of two ovaries. However, the frequency of ovulation decreases some years before the menopause. The oocyte enters the uterine tube, where it may be fertilized by one of the millions of spermatozoa or sperm deposited into the vagina by her sexual partner. The nucleus of the oocyte and that of the spermatozoon (the gametes) each has 23 chromosomes (the genetic material), so that when they merge forming a zygote at conception or fertilization, the normal human complement of 46 chromosomes per cell is usually restored. Thus an individual receives half of their genes from each of their parents.
After 24–36 hours, the first cell division occurs, and mitosis continues rapidly. Within 3 days a cluster of cells is formed, about the size of a pinhead. During the second week, the cluster of developing cells implants into the specially prepared lining of the uterus known as the decidua, which will provide nourishment until the development of the placenta. The term embryo is used from the early developmental stages until the eighth week of pregnancy (gestation). Thereafter, until birth it is known as a fetus.
The cluster of cells continues to develop and will eventually differentiate into all the specialized cells of the human body. Occurring alongside these events are the processes that result in the formation of two protec-tive membranes, the chorion and amnion that enclose the embryo/fetus, the umbilical cord and the placenta. The amnion contains the amniotic fluid in which the developing fetus floats throughout pregnancy. The placenta, which has close contact with maternal blood vessels in the uterus, delivers oxygen and nutrients to and removes waste from the fetus through blood vessels in the umbil-ical cord via the adapted fetal circulation of vessels and shunts that mostly bypasses the lungs and gastro-intestinal tract. These adaptations are normally reversed soon after birth.
During the early weeks after implantation, all the organ systems start to develop, so that a heart beat, lungs and limbs are detectable within 4 weeks, and the eyes, ears, nose and mouth as well as rudimentary digits can be visualized after 8 weeks of pregnancy. At this early stage, the embryo is particularly vulnerable to adverse factors such as toxins and microorganisms, and these may have major effects on developing organs, e.g. the rubella virus may cause heart defects and deafness.
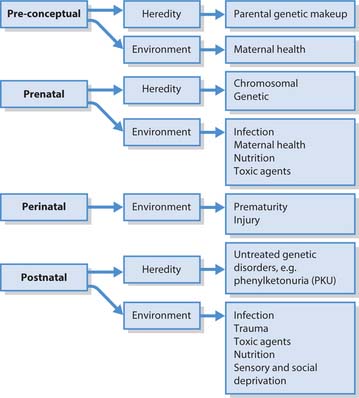
There are many possible causes of learning disabilities, either genetic (hereditary) or environmental (Fig. 8.2), which can occur during different stages of development. These include:
Down’s syndrome
A friend and her partner are planning to have a baby and she asks you what causes Down’s syndrome and the risk of having a baby with Down’s syndrome. She also asks what diagnostic tests are available during pregnancy.
Student activities
[Resources: Down’s Syndrome Association – www.downs-syndrome.org.uk; Down’s Syndrome Scotland – www.dsscotland.org.uk; UK National Screening Committee: Down’s Syndrome Screening Programme NHS – www.screening.nhs.uk/downs/home.htm All available July 2006]
From the end of the second month to the end of pregnancy (usually 40 weeks) the fetus grows from 2.5 cm in length and 7 g in weight to around 50 cm and over 3500 g. Sex can be ascertained after 3 months, while development of the brain, lungs and heart make viability possible from about 24 weeks of gestation (Bee & Boyd 2004). Detailed information about fetal development can be found in Further reading (e.g. Chamley et al 2005).
Infancy (0–12 months) (see also ‘Developmental milestones’, pp. 201–203)
Although infants typically lose some weight in the days immediately following birth, once feeding and digestive processes are established, growth is extremely rapid, with up to 0.5 kg being gained per week, so that birth weight is doubled on average by the age of 18 weeks. Similarly, an infant can increase in length by 1 cm over a single week during this stage.
The first teeth start to erupt around 6 months of age (see Ch. 16); a delay in the eruption of teeth may be an indicator of other developmental problems.
Motor strength and coordination also steadily advance during infancy. The head is disproportionately large, and requires a steadying hand to support it in the neonatal period (first 28 days). However, by 8–12 weeks, the infant’s neck muscles are able to prevent the head lolling backwards, and by 9–12 months the infant can sit and latterly stand unaided.
Mobility also increases: by 3–6 months, the infant should be able to roll over, crawl by 6–9 months and some infants can walk well by 12 months.
Childhood (1–10 years)
The rate of growth slows, but by the age of 2–3 years, children attain half their adult height, although less than one-fifth of their healthy adult weight.
During the preschool period, up to 5 years of age, there are continuing increases in size and strength, accompanied by apparently boundless energy, and punctuated by the appearance of skilled behaviours such as doing up buttons (see also ‘Developmental milestones’, pp. 201–203).
For further detail of growth during childhood the reader is referred to Further reading (e.g. Montague et al 2005).
Adolescence (11–18 years)
During adolescence, the period between the onset of puberty and adulthood, further growth spurts are stimu-lated by the sex hormones oestrogen and testosterone (see Table 8.1). These episodes of sudden growth may pose challenges in relation to coordination of a typically gangling frame. At the same time, self-consciousness is further increased by the appearance of secondary sexual characteristics (Box 8.16) with inherent and unavoidable challenges to self-image (see p. 201).
Younger adulthood (18–40 years)
Early in this stage, most people reach their maximum height, because the epiphyseal plates (cartilage) of long bones become bone (ossify), thus preventing further growth in stature. However, growth in height may cease earlier in young women. It is important to maximize bone density during the teens and twenties (Box 8.17, p. 200). Bone mass peaks during the late twenties but after 35–40 years of age it starts to decline. Not only are individuals now at their peak of skeletal muscle bulk and physical strength, speed and athletic potential, but the cardiovascular system also possesses its maximum oxygen-carrying capacity and immune responses are at their peak, so that young adults recover quickly from exercise, injury and illness. Brain mass and sensory powers are similarly at their highest point, resulting in optimal ability to discriminate stimuli.
 HEALTH PROMOTION
HEALTH PROMOTIONEating disorders and bone density
Eating disorders such as anorexia and bulimia nervosa can have far-reaching consequences for bone health. Apart from an inadequate intake of the nutrients needed for bone growth and density (e.g. calcium, vitamin D, protein, etc.), there are other issues for young women with eating disorders. Those with a very low body weight may stop having periods and the lack of oestrogen puts them at risk of loss of bone density, which may never be rectified even if they gain weight and their periods return. This may also occur when young women exercise excessively with or without an eating disorder. Loss of bone density or a failure to reach peak density increases the risk of osteoporosis (see Ch. 18).
[Resource: National Osteoporosis Society – www.nos.org.uk Available July 2006]
The middle years (40–65 years)
Most adults in Western society can currently look forward to living well into their seventies or eighties, owing to reduced mortality from disease, occupational accidents, etc. compared with past generations (see Ch. 1). By the mid-forties there are usually detectable, but not serious, signs of decline in all body systems (Box 8.18).
Box 8.18 Changes in body systems in middle years
The integumentary system
The senses
Cardiovascular and respiratory systems
Body weight in middle years
The reproductive system
Even into their fifties, however, many people consider themselves healthy and if no longer in their physical prime, not far short of their best in terms of intellectual and social functioning – their ‘prime of life’.
Older adulthood
Beyond the relative physical and functional plateau that extends from young adulthood to middle-age, individuals must progressively adapt to the more obvious changes that accompany ageing, often exaggerations of those which start to appear in the middle years.
As indicated by Mader (2000), physical aspects include:
Functional aspects typically include more troublesome reductions in:
However, although the incidence of illness and disability does increase with age, most older people, especially those under 75 years, are healthy and independent. They retain their mental faculties and continue to enjoy life, especially if they can reconcile themselves to adapting to their relative limitations. Although the proportion of older people in Western society is increasing, health-related factors such as diet, housing, technological and medical advances may allow their prospects to be brighter than for previous generations.
Developmental milestones
Human development is often thought of as a process involving the achievement of competencies or ‘milestones’, i.e. the ability to perform tasks that society expects of its members at a given point of their lives. Such competencies are progressively acquired during physical mat-uration (increasing age, size, strength and coordination) and through opportunities for practice. Development is therefore viewed as a complex interplay of biological, environmental and social factors.
The usual way of assessing an infant’s/child’s developmental progress is to compare their behaviours with those displayed by the majority of their contemporaries. Following detailed studies, abilities have been organized into comparative grids, for example the Denver II (1990) (Fig. 8.3), which divides infant’s/children’s milestones into four categories:
Fig. 8.3 The Denver II (1990) Developmental rating scale.
Copyright 1969, 1989, 1990. WK Frankenburg and JB Dodds; copyright 1978 WK Frankenburg (reproduced by kind permission of Denver Developmental Materials Inc.)
Cross-comparison can establish whether a particular infant/child has attained a series of milestones established as typical for their age. This is a matter of concern to many parents, but it should be appreciated that compiling ‘average’ scores involves rating some children as showing behaviour relatively early or late. Significance is only really attached to this if all related behaviours or overall progress follows the same pattern. Additionally, it is common for children to be advanced in some abilities and delayed in others, and for boys and girls to develop at slightly different rates (Box 8.19, p. 204).
Developmental assessment
In order to detect problems at an early stage, it is important to assess the progress of infants and children in attaining certain milestones, such as smiling or building a tower of bricks.
Student activities
Psychosocial development
This refers to the psychological and sociological perspectives on the process of development. The stages are considered by age group.
Infancy and childhood
The main issues relating to infancy are considered under self-concept and attachment below.
Early in childhood, preschool milestones must be attained, a process that may in some instances occur naturally, but in others such milestones are awaited anxiously and require greater facilitation. By the age of 5, children are required to attend school, mix with peers and accept direction from unrelated adults (see ‘Socialization’, p. 195), an experience that can initially prove traumatic.
As mentioned above, young children possess enormous energy (to be expended in a shorter day than their parents’/carers’ reserves) as well as steadily increasing bodily strength and frame size. Awareness of this potential power, constrained by restrictions imposed by adults and accentuated by intense emotions, can lead to behavioural problems. These range from the tantrums of the ‘terrible twos’ to destructive rages, scuffles and vandalism in school years. Such features can be pronounced in the behaviour of some young people with learning disabilities, whose psychological resources may be overstretched at times by the demands of normalization, i.e. adapting to the myriad stresses of life lived within mainstream society. In these situations it is important that parents/carers consider what is being communicated or how the environment can be adapted.
Adolescence
The physical changes during puberty generate psychosocial challenges for the adolescent, who must come to terms with new experiences, including:
All this is accompanied by concurrent cognitive, e.g. scholastic, and ethical developments that will be con-sidered later. Teenagers tend to be acutely aware of their bodily appearance and hygiene (taking much time over self-care), and concerned about issues of modesty and privacy, relevant to those nursing them. By the late teenage years many individuals have reached their highpoint in terms of physical suppleness, speed and reproductive ability, but outlets for these may be limited and external constraints resented.
Young adulthood
This phase is usually considered to begin around 20 years of age, although attainment of adulthood may be culturally defined in various ways, for example:
The nervous system functions at its peak, resulting in optimal ability to detect and memorize information, and to solve problems. Physical attractiveness is often regarded as most striking at this time. Consequently, self-confidence may simultaneously expand. While each of these attributes may gradually diminish from the age of 26 onwards, factors such as experience, reasoning ability and motivation may more than compensate.
The middle years
A common psychological challenge for women in their mid-forties to fifties is the ‘empty nest syndrome’, having to adjust to their children entering young adulthood and leaving home. This can prompt women to re-enter the labour market or restart their career, which, not uncommonly, coincides with marital separation or divorce. Career opportunities can, however, be offset by the need to provide care for older relatives. Childless women also come to the realization that they are now unlikely to have a child.
Male awareness of sexual difficulties, occupational and relationship stagnation, perhaps compared with their spouse’s new lease of life, and of approaching mortality can combine to precipitate the ‘male menopause’, either expressed in introverted self-doubt or the purchase of a Harley–Davidson motorcycle.
Older adulthood
Psychological aspects of old age are well documented (Gross 2001). These may include diminished ability to solve new problems, memorize and retrieve information. As all of the above changes seem to be negative and relate to loss, perhaps it is unsurprising that depression is relatively common in older adults, and the prospect of ageing may be ignored, dreaded or defused through humour.
Retirement can also be a rewarding period where the person has more time to devote to relationships, e.g. with partners, children, grandchildren and friends, hobbies and part-time or voluntary work. Lifestyles associated with contentment in old age vary between authorities, for instance the contrast between ‘disengagement’ and ‘activity’ models (Gross 2001).
The ‘self’ and ‘self-concept’
These terms are often used interchangeably when examining how people think about themselves, and consider their own nature and actions. This process is also referred to as ‘self-awareness’ or ‘self-consciousness’. It might be viewed as a straightforward, natural part of a person’s existence, but the ‘self’ is a complex notion, unique to human beings, which they have to develop and continuously modify throughout their lives. It involves forming the ability to take the role of subject and object, observer and observed, at the same time. Self-consciousness is particularly intense when a person is especially aware of being viewed as an object, for example suddenly finding themselves in front of a group of ‘spectators’, such as when arriving late for a class (Box 8.20).
Possible instances might include:
The self can be conceived as comprising three interrelated elements: self-image, self-esteem and ideal self.
Self-image
The first of these is effectively the impression people hold of them, and includes how they think that they appear outwardly to others and the kind of person that they believe they are (Box 8.21).
The TST
One way of investigating a person’s self-image would be to ask people to describe themselves. Kuhn and McPartland in their ‘twenty statements test’ (TST) used this approach in 1954.
Personality traits
These are adjectives that allow people to subjectively describe their mental processes such as thoughts and feelings, or their behaviour. Examples might include ‘I am… kind, caring, practical, hard working, which are all good characteristics for a nurse, outgoing or shy. Sometimes these can be grouped to form a so-called personality ‘type’, for example traits such as ‘shy and retiring’, ‘thoughtful’, ‘serious’ and ‘cautious’ may combine to constitute an introvert, contrasting descriptions such as ‘sociable’, ‘lively’, ‘fun-loving’ and ‘impulsive’ relating to the opposite extrovert type (Eysenck 2000). Eysenck (senior)’s, other main distinctions were between:
Trait and type approaches to self-description are commonly used in everyday language as well as in psychological research, and imply that aspects of the self are relatively fixed once established, and can be compared and contrasted between individuals, e.g. colleagues or clients.
Roles (see pp. 195–196)
Such answers may include familial roles such as ‘mother’, ‘daughter’, ‘aunt’ or ‘sister’, or occupational ones such as ‘student’, ‘nurse’ or ‘doctor’. Also common may be statements of religious identity, e.g. ‘I am a ‘Christian’ or ‘Muslim’.
Factual
Factual matters include gender, marital status and age (perhaps commoner if the respondent is towards the extremes of lifespan). Literal answers are characteristic of younger age groups, for instance children under 8 years tend to answer the TST in terms of activities, e.g. ‘I am playing’, ‘… at school’, or even ‘… talking to you!’ Between 8 years and adolescence, answers usually revolve around facts such as their:
(Miell 1990).
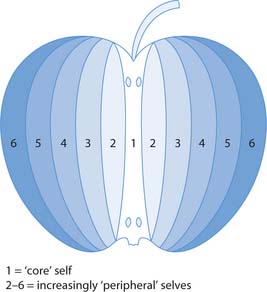
The relative importance of a person’s TST answers can be gauged by asking them to rank each in order of importance. This then enables the construction of a concentric model of the self-image (Fig. 8.4), with the central one representing the most important self-descriptor and the true ‘core- self’, compared with the progressively less important ‘peripheral- selves’ outside this.
Physical characteristics, such as size or appearance, form part of the ‘bodily self’, or ‘body image’, and may appear in response to the TST if perceived to be a particularly significant part of the outward self. The bodily self also includes sensations such as hunger, thirst, satiety, warmth, cold, pleasure and pain – common preoccupations during ill-health, and which help to direct conscious awareness towards survival-related actions. It also covers anatomical components (body structure), which might be automatically regarded as an, or indeed the essential part of people’s living selves, although they lose parts of it without concern, as when cutting their hair and nails. Possession of bodily parts or even fluids can be an ambiva-lent matter, e.g. when considering donating or receiving organs or blood.
However, there will be circumstances where an adolescent or adult patient/client would particularly fixate on the bodily self when responding to the TST. For example, chronic pain, preoccupation with weight in anorexia nervosa or obesity, disfiguring burns, paralysis, loss of continence, breast removal or stoma-forming surgery, and depression may engender self-loathing.
Self-esteem
The ability to evaluate their self-image leads people to examine the second component of the self – their ‘self-esteem’. This is how people feel about the image they hold of themselves, the degree to which it pleases or displeases them, and whether they take pride in or feel shame towards it. Thus people can run a range of emotions when appraising themselves, from conceit to despair with all points between these extremes, and these judgements vary with time, their behaviour and circumstances. This self-evaluation may be directed at specific aspects of the self, for instance appearance, thoughts about issues or other people, emotions such as desires, or actions that have been performed. Alternatively, it may be a ‘global’ amalgamation of such detailed appraisals, generating an overall estimation of self-value at a given moment.
Self-esteem is enormously influenced by the culture to which people belong. Western culture is often said to value material wealth and individual attainment. Thus an individual member of this society is likely to have their self-esteem bolstered by financial security, ownership of impressive clothes, house and car, academic qualifications and a high status job, many of which can be contingent on each other. Absence of such indicators of personal success is liable to lower a person’s self-esteem, unless they belong to a non-materialistic subculture, e.g. a religious organization or an anti-capitalist protest group, from which they may derive a quite different yardstick of personal worth.
Self-esteem clearly has a major bearing on emotional well-being and so is integral to personal happiness. If people aim to be personally fulfilled and happy, this seems to imply a potentially aspirational element to the self-concept. If self-image represents the ‘person’ that people consider themselves to be, sometimes termed the ‘actual self’, it may not be all they would like to be or could be. The wished-for improved version was termed the ‘ideal self’ by Rogers (see p. 184). Another way of tackling the problem of lowered self-esteem is to avoid exacerbating factors. People often evaluate their self-image by comparing themselves with others. If inappropriately successful figures are chosen for reference purposes, it is likely that disappointment will ensue, for example, comparing one’s physical attractiveness with that of a film star or one’s material success with a millionaire. Similarly, a student nurse is liable to feel inferior in poise and skills to an experienced registered nurse.
William James suggested a formula akin to:

In other words, the higher their expectations, the more likely they are to exceed the person’s achievements, and the likelier they are to be disappointed. This indicates some need to be realistic in personal targets, e.g. the goals negotiated with a patient/client for their rehabilitation, although equally it could be argued that without aspirations people are unlikely to improve themselves or achieve anything significant in their lives. Rearranging the formula gives:

Therefore, harbouring high self-regard and goals is likely to make people more successful, so that a positive view of the present and future self may be conducive to generating good fortune, e.g. in a student’s nursing career aims.
Development of the self
As people are not born with an intact, innate self-concept, how is it formed? Piaget (p. 207) proposed that the infant below the age of 6 months is egocentric or self-centred in that they are unaware that a world separate from themselves actually exists. It takes at least a further year to create an understanding of the reality of the surrounding environment, including the people within it. Work on object permanence (see p. 208) suggests that young children only develop a consistent interest in (which implies a concept of) absent things and people, i.e. the ‘not self’, by about 18 months. Furthermore, research by Lewis and Brooks-Gunn in the late 1970s suggested that only above this age do children recognize their own image, for instance in a photograph or their reflection in a mirror, as distinct from images of other children of the same age.
This work followed up findings by Gallup in the early 1970s on primates, which found that only higher apes seemed able to develop similar self-recognition, and only then if they had been exposed previously and early in life to other members of their own species. This usually occurs naturally, and seems essential to future social functioning such as mating and parenting (see attachment, pp. 212–214). On the basis of his results, Gallup asserted that the self is ‘a social structure, and arises through social experience’. In other words, humans at least begin to form their self-image through being reared by other humans, and gradually recognize their form as similar to those of the children and adults they see around them, until they can conceive their own physical boundaries and appearance towards the end of their second year of life.
From early infancy, children naturally interact with those around them, initially exchanging gaze and facial expressions like smiling with their mother, then during their second year beginning to use recognizable words of their ‘mother tongue’. Such symbols, along with gestures such as waving, provide the means of communicating shared meanings during interpersonal interactions, the basis for what is termed the ‘social interactionist’ perspective, initiated by George Herbert Mead in the 1930s. Mead developed the observations made in the 1890s by William James on the linguistic distinction between the terms ‘I’ and ‘me’ – both in this context sometimes given the prefix ‘the’. The first-person pronoun ‘I’ is used to denote the self as the subject of the act of thought, speech or behaviour. James likened this to a knowing but hidden observer, almost like an ever-alert motion camera, placed within what he termed a person’s ‘stream of consciousness’. This ‘I’ might be equivalent to the essential ‘core- self’ referred to earlier, a secret entity in some ways, unattainable even to its owner.
On the other hand, the pronoun ‘me’ refers to the self when viewed or treated as an object, and amounts to what in a person is outwardly observable, such as their physical appearance, clothes (e.g. when you ask another person whether a new coat is ‘me’ or ‘not me’), overt behaviour and even reputation. This use of ‘me’ in speech has already been noted in relation to the bodily image, and its evaluation is much affected by social influences such as the perceived or anticipated opinions of others. Thus the ‘me’ may be modified in order to maximize one’s self-esteem, and it is the ‘I’ in this framework that makes these judgements and decisions.
Although fully understanding the social interactionist argument with its peculiar linguistic interrelations is challenging, it suggests that once consistently mastering the use of the terms ‘I’ and ‘me’, the child must be displaying awareness of the parallel existence of both ‘self’ and others, and how their standpoint and those of other people interacts.
As well as through the acquisition of language skills, Mead contended that the self-concept developed by means of assuming roles. He described three stages of his own conception of ‘primary socialization’ (see p. 195) during which this occurred. In the initial preparatory stage, the young child can be seen closely imitating parental actions, such as washing dishes and vacuum cleaning. At this time, the child is very sensitive to parental feedback, whether encouraging or disapproving, and internalizes their judgements (Miell 1990).
In the second stage, play often involves the re-enactment of adult behaviour when the child is alone, frequently accompanied by a commentary conveying previously expressed parental attitudes, such as praise or criticism of what a toy is being made to do.
Finally, by participating in relatively formal games, the older child has to adhere to rules established by others. To be successful, the child must learn to take the viewpoint of others, both on their side and in opposition, for instance in cards or ball games, in order to anticipate what the others are likely to do. Thus, through each stage, the child engages more and more with the viewpoints of other people, developing the power of empathy. Eventually they are able to appreciate the typical perspective of those within their culture, for example what the average person might think of their thoughts, appearance and behaviour (Cooley’s looking-glass ‘self’). Mead termed this adoption of the ‘role of the generalized other’, and this ability provides a yardstick against which to evaluate one’s self or a virtual mirror to reflect one’s self-image as viewed by others. This limitless source of socially grounded feedback enables the person to subtly and continuously modify and refine their ‘selves’ throughout life, both in later interactions with the agents of secondary socialization (p. 195) and in moments of solitary ‘self-reflection’.
Refinement of self in adulthood occurs during ‘pro-fessional’ or ‘tertiary’ socialization, whereby people acquire the knowledge, skills and attitudes peculiar to an occupational role (p. 195). Goffman (1971) described the process of assuming the behavioural component of such a role in terms of taking part in a drama. Initially an actor may feel not entirely natural in a part, and uncertain about how convincingly they can fulfil a well-established role, just as a student might that of ‘nurse’. A professional ‘mask’ is self-consciously adopted to begin with, and feedback gained on performance from observers, e.g. mentor. Aspects of performance can be modified until the person feels confident about fulfilling the role’s requirements and can routinely ‘play’ it naturally.
To summarize, the ‘self’ is an elusive and vague concept. It comprises psychological and physical components that are interrelated. People develop their self-concept in the course of continuing social experience, through their interactions with others. Their view of themselves is much influenced by the culture in which they exist, and the reactions to them of the people they encounter, both real and imagined. The self-concept is fluid; they can adapt their ‘selves’ to varying situations, such as behaving quite differently in professional and domestic roles. Lastly, because of the tendency to constantly evaluate the self-image, which generates conscious self-esteem, the self-concept is crucial in determining a person’s emotional well-being – it is intrinsic to their inner contentment.
Cognitive (intellectual) development
The most influential researcher in this field has been the Swiss psychologist Jean Piaget (1896–1980) who worked on the development of early intelligence tests. These instruments implicitly assume that intelligence is an attribute determined at birth, or early in life, and unchanging thereafter, and that it can be estimated through standardized questions. Rather than taking this usual focus, Piaget became fascinated with children’s typically incorrect answers to items beyond their chronological ability. He felt that these yielded unique insights, as they reflected the characteristic, if immature, ways in which children think. Consequently, he devised a series of tests specifically designed to shed light on intellectual processes at different ages.
Piaget believed that human understanding of reality was not inborn, but had to be actively ‘discovered’ through interactions with the real, outside world, the child effectively learning as a scientist would. In other words, intelligence ‘evolves’, just like the characteristics of a species in response to environmental challenges, ensuring survival and success. Initially, reflexes (‘automatic’ responses) suffice in these interactions, so that the infant can both derive nourishment from its mother’s breast or a bottle teat and investigate objects such as toys through automatic sucking and licking. A psychologically comforting state of ‘equilibrium’ results through being able to ‘accommodate’ or successfully respond to every encountered challenge by existing strategies – ‘schemata’ (singular schema) are the building blocks of Piagetian intelligence. However, the growing infant comes to find sucking and licking less successful in dealing with solid food or unpleasant-tasting objects that they handle, resulting in inner dissatisfaction or ‘disequilibrium’. This necessitates the formation of new strategies, such as biting and chewing food, scrutinizing and fingering objects, better suited to new challenges – the process of ‘accommodation’. According to Piaget, this continuous process, known as ‘equilibration’, of employing old schemata until they fail and then replacing them with new, more suitable ones characterizes adaptation, and so intellectual development, throughout life (Fig. 8.5).
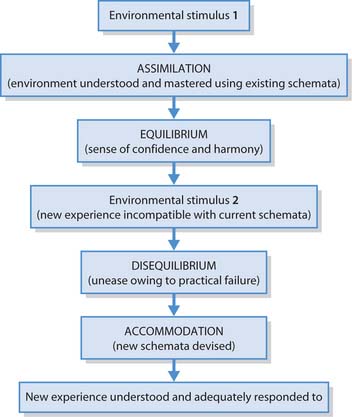
Assimilation allows people to practise recently acquired skills, e.g. in nursing, until they achieve routine competence in them. Accommodation enables people to formulate innovative approaches towards solving new problems. Both processes are thus complementary and integral to lifelong learning and the development of the mastery that characterizes the expert nurse.
An everyday example might be being offered chopsticks for the first time in a Chinese restaurant, where a person might try them, especially if everyone else around does. Assimilation would involve trying to use the sticks as a blunt spoon, attempting to scoop the food up with them. Much of it, especially the rice and sauce, will fall before it reaches their mouth, creating embarrassment and frustration (disequilibrium). With practice, the person learns to move each chopstick separately, allowing the tips to grasp food securely (accommodation). Success makes the person feel competent and appeases their hunger (equilibrium). Feeding dependent patients also involves new strategies, such as prior consideration of comfort, hygiene and dignity, then asking them in what sequence or mixtures they would like their food, when they might like a drink and observing repeatedly when their mouth is empty. All of these strategies occur automatically when people can feed themselves (adapted from Napier University Module booklet 2, 1997, 2001).
Piaget’s four stages of cognitive development
Piaget contended that children invariably progress through four consecutive stages en route to acquiring an adult intellect. Each stage has its own characteristic schemata, way of thinking or intelligence.
Piaget envisaged intellectual development as proceeding continuously through the stages, driven but also limited by accumulating experience and biological maturation. His ideas have received considerable cross-cultural confirmation, although a number of studies have suggested the need for revision of the details.
Criticisms have been directed at:
Sensorimotor stage (0–2 years)
This stage is so-named as the infant’s ‘thinking’ appears limited to sensing events and objects, and reacting to them by muscular movements, e.g. reaching for rattles, crying if wet. As a result, sensorimotor intelligence is ‘practical’, as the infant is reacting only to circumstances and objects that are evident to them. It takes some months for the infant to show awareness of absent things, such as searching for objects that are hidden or made to disappear, even if they witness their disappearance. This convinced Piaget that ‘object permanence’, i.e. that people and objects have an independent and permanent existence of their own, separate from the infant, has to be developed through experience. Piaget described the infant yet to acquire this notion as in a state of pure ‘egocentrism’.
By about 18 months, the child starts to use symbols to represent absent people and objects, such as words, imitative behaviour and toys. Thus they will ask for Mum or a favourite cuddly toy by name, re-enact behaviour previously exhibited by a parent or sibling (‘deferred imitation’) and use a building brick as if it were a car in representational or ‘make-believe’ play.
Preoperational stage (2–7 years)
The child continues to improve in use of language and other symbols, but tends to be convinced, and confused, by how things outwardly appear rather than by operating on the basis of logic, i.e. logical ‘operations’ do not yet characterize thought. Thus during the first 2 years of this stage, the ‘preconceptual’ substage, the child focuses or ‘centres’ on one striking aspect of an object to the exclusion of other relevancies. So adult males of similar age and appearance may be indiscriminately called Daddy, and four-legged animals of a certain size, from cats to Shetland ponies may be called ‘doggies’. Inanimate objects that move, like the sun and moon, cars or footballs are viewed as living.
By 4 years of age, the child progresses to the ‘intuitive’ substage, where some logic is present but intuitive thought, relying on what feels right, make cross-classification or ‘class-inclusion’ tasks difficult. An example is the comparison of toy cows, e.g. either white or black in colour. Identifying the more numerous colour is easy, but these are also thought to outnumber the total number of toy cows. However, this might be due to the lack of prac-tical relevance of the task to a small child. In the 1970s, Donaldson showed children the cows with some standing and others on their side, which were said to be ‘sleeping’. It seemed easy for them then to judge that ‘all’ cows outnumbered ‘sleeping’ cows.
Before 7 years of age, the child still displays egocentrism, but in a lesser form than in the sensorimotor stage, equivalent here to a relative inability to see a situation from anyone else’s standpoint. For instance, the child will know if they have a brother, can tell you this brother’s name, yet may insist their brother does not have a brother or sister of his own. Children who should by age be markedly egocentric can sometimes perform empathetic skills such as ‘talking down’ to and selecting suitable toys for 2 year olds, which inexperienced adults might find difficult (Box 8.22), or understanding that keeping a secret means that others are excluded from this knowledge.
Safety in play – choosing the right toy
Toy manufacturers typically specify if their products are unsuitable for children less than 3 years of age, as small components may cause choking (see Ch. 17).
Student activities
Concrete operational stage (7–11 years)
After entering this stage, children become able to solve previously tricky logical operations such as ‘conservation tasks’. For example, they can be confronted with two identical short, broad tumblers, and invited to judge when both are filled with milk to the same level. The content of one of these is then poured into a taller glass as the child watches. The child is then asked if there is now the same in it as in the other original broad tumbler, or whether there is less or more. Piaget thought that the essential indicator of attaining this stage was to agree that they were the same. By focusing on more than one feature simultaneously, ‘decentring’, one can understand that height compensates for breadth so that milk transferred to a different-shaped container conserves its volume and its physical identity, despite its changed appearance. Preoperational children insist that the tall glass has more even if they agree that none was spilled in transfer. Other measures of conservation ability relate to substance and number.
One criticism of this research questions the significance of the word more – for a child below 7 years, does the term simply mean receiving a higher level of milk or juice in a glass, suggesting that the preoperational immaturity may be linguistic rather than logical? Another relates to the method of questioning and the power relationship between experimenter and respondent. How might a child interpret an adult repeating the question, ‘Are both the same or does one have more?’ after rearranging the test items? Perhaps a child might feel that they should ignore what is logically correct, maybe suspecting some magical trickery, or that they should change their answer to the question second time around, as this is what the grown-up presumably expects if asking it twice.
Finally, relative terms such as big, bigger and biggest, previously used interchangeably, are employed appropriately from now on, allowing accurate verbal comparison between two or more objects. The stage gets its name from the observation that the newly characteristic logical strategies are reliably used only when the components of the problem can be seen and perhaps touched, i.e. they have a concrete presence.
Formal operational stage (11–15+ years)
This refers to the ability to follow the form or theore-tical outline of a problem when remote from its physical reality or lacking a concrete context. Examples include following verbal or written instructions rather than observing then imitating someone showing you how to do something, or being able to delay implementation of new learning. Comparing two absent objects such as people described independently of one another becomes straightforward, e.g. ‘if John is taller than Mary, and Jim is smaller than Mary, is Jim or John the tallest?’ – a transitivity test, requiring correct use of relative terms.
Logic can now thus be applied in an abstract way, making future practical applications easier, since general principles can be applied to many different situations, as in linking nursing theory to subsequent practice settings. The contrast between formal and concrete operational thinking is akin to that between insight and behavioural or social learning (Ch. 4). However, there is some doubt if all or even most adults are able to function consistently at this level, as adults may persist in using unsuitable trial and error or observational approaches to tasks that could be solved by creative, abstract thinking, sometimes with frustrating results. For example, when setting up unfamiliar equipment, some people push buttons randomly or ask another’s opinion, rather than consulting the instructions.
Hypothetical thinking enables consideration of (im)possibilities, e.g. science fiction, surreal humour and alternative courses of action, which leads to some of the conflicts that typify adolescence, including friction with elders, personal identity crises and vacillation over career choice.
Formal operational thought requires attainment of the highest level of thinking in Piaget’s model. People with learning (intellectual) disabilities may have particular difficulty using and relating to formal operational thinking, as it requires intellectual ability at the level of secondary school age. Thus they may benefit more from practical demonstrations and supervised experience, e.g. in living skills and health promotion, compared with more abstract methods such as verbal or written explanation (Box 8.23).
Health promotion for different stages of cognitive development
Nurses in all areas of practice have an important health-promoting role. However, effective health-promoting initiatives require careful planning, which considers the person’s/group’s stage of cognitive development.
Student activities
[Resource: Department of Health 2006 Essence of care. Patient-focused benchmarking for health care practitioners. Online: www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4005475&chk=A0A4iz Available July 2006]
Box 8.24 provides an opportunity to consider what children can do, and relates practical observations to Piaget’s four stages.
What can children do?
A series of practical, age-related activities are provided for you to use.
3–15 months
Hide a toy behind a cushion. Observe if the child tries to search behind it. If they do, move it behind an adjacent cushion. Usually this occurs from about 8 months, but the child is easily ‘fooled’ if the hiding place is discreetly changed, and will not persist with their search until into their second year.
2–3 years
Find out whether the child can consistently distinguish between different animals, perhaps using a picture book or visiting a zoo.
4–5 years
See if the child can play hide-and-seek, a game that requires participants to imagine where others would conceal themselves to avoid detection.
9–14 years
Ask the young person, ‘What would happen if people could fly?’ In the concrete operational phase this is either considered seriously or answered in a literal manner, e.g. ‘That would be fun’, ‘Where would our wings be attached’ or ‘Don’t be silly’. Those at the formal operations stage are likely to be flippant, and suggest ‘You could sleep longer before school’ or ‘It might save fossil fuels’. In other words, the answers reflect the differences between the literal reaction of children to science fiction and fantasy, viewing supernatural powers as something to emulate, and adults’ intrigue with the interesting notions involved and their possible ethical ramifications.
Alternative theories of intellectual development
Jerome Bruner studied the changing ways in which the child represents the world. Initially in the ‘enactive’ stage this is through actions, such as motor responses, akin to Piaget’s sensorimotor stage. Then in the ‘iconic’ stage, formation of mental images becomes paramount, roughly equivalent to the preoccupation with appearances in Piaget’s preoperational stage. Finally, around 7 years of age, the ‘symbolic’ stage commences, in which use of and growing sophistication of language directs thought and its development. Piaget preferred to regard changes in use of language as reflecting rather than engineering an individual’s cognitive advances. Research, e.g. deaf children whose language skills are typically delayed more than their thinking abilities, tends to support his opinion.
In the 1930s, Lev Vygotsky had also argued the import-ance of inner speech or verbal thought in development. He considered that this and other forms of social activity were instrumental in encouraging problem solving and self-sufficiency. For example, an adult may tutor a child in a task such as putting on clothing through either general advice or specific prompts, providing the ‘apprentice’ with the ‘scaffolding’ of another’s experience, so accelerating mastery. Student nurses can similarly benefit from the practical expertise passed on by mentors. Cultural learning is similarly imparted between generations by interpersonal means (p. 195), and people’s most highly developed cognitive skills tend to relate directly to those valued by the society to which they belong (Gross 2001).
Cognitive approaches to moral development
As with intellect, cognitive approaches regard morality as developing progressively and consciously during childhood and adolescence through a predictable succession of stages, each as distinctive as those relating to other forms of thought.
In Piaget’s view, 5–9 year olds conceive morality as an absolute system of rules and sanctions directed by higher adult authorities, ‘external’ morality, demanding one-sided respect, to whom obedience is a virtue in itself, termed ‘moral realism’. Those over 10 years increasingly feel more constrained by their own principles of right and wrong, ‘internal’ morality, which evolve through respectful mutual negotiation. Thus lying to an adult is viewed as no worse than doing so to a peer. Understanding and respecting the viewpoints of others becomes an ethical prerequisite of trusting social relationships, ‘moral relativism’. Piaget considered that these qualitative moral changes result from, and so lag behind, the cognitive transformations, e.g. the ability to decentre and reduced egocentrism, which typify the attainment of operational thought.
Kohlberg’s work
In the mid 1950s, Lawrence Kohlberg designed nine scen-arios involving moral dilemmas, i.e. problems involving at least two ethical principles that are impossible to resolve completely satisfactorily (see Ch. 7). The most famous of these is provided in Box 8.25.
A moral dilemma
Somewhere in Europe, a woman was dying from cancer. One drug might save her, newly discovered by a pharmacist working in the same town. The pharmacist was charging 10 times what the drug cost him to make. The sick woman’s husband, Heinz, went everywhere he knew to borrow the money needed to purchase the medication, but he could gather only about half of the cost. He told the pharmacist that his wife was dying and asked him to sell it for less or let him pay later, but the answer was a firm ‘no’. Heinz became desperate and broke in to steal the drug for his wife.
What interested Kohlberg was the rationale given for favouring one course of action over another. Analysis of his subjects’ responses led him to formulate a theory that individuals can progress through three levels of moral development, each comprising two substages and, like Piaget’s types of morality, contingent on preceding intellectual advances (Box 8.26).
Either basic response to Heinz’s and to the other dilemmas that Kohlberg devised, i.e. whether Heinz should or should not have stolen the drug, can be fitted into Box 8.26, depending on the reasoning given for the judgement, allowing the respondent’s stage of moral development to be inferred. Some examples are provided in Table 8.2.
Table 8.2 Rationale at various levels of moral development for Heinz scenario (see Box 8.25)
| Stage | For stealing the drug | Against stealing the drug |
|---|---|---|
| 1 | Heinz may not be caught or convicted | Heinz is the likely suspect and will probably be imprisoned |
| 2 | Heinz’s wife and family will love him for his devotion | Heinz may face a fine he can’t afford or lose his job for being convicted |
| 3 | A public outcry would follow in support of him | Significant others whom Heinz respects may disapprove of his actions |
| 4 | Heinz would be fulfilling his duty of care to his wife | Flouting the law may generally erode its social authority |
| 5 | A legal test-case could follow, resulting in a change in the law | Technically theft is illegal, no matter what an individual’ motive behind it |
| 6 | The principle of respecting life takes precedence over property | The pharmacist’s rights have been infringed, and future research deterred |
Kohlberg reported that only 20% of adults are governed by ‘post-conventional’ morality and just 10–15% operate on the most advanced level. This finding may be related to the limited proportion of adults who consistently demonstrate Piaget’s stage of formal operational thought. As well as advancing through cumulative reasoning ability, Kohlberg thought that morality developed alongside biological maturation and practical challenges inevitable in new social experiences. His work has received criticism on the basis of his research methods (seen as both subject-ive and abstract) and his implicit assumptions, e.g. that ‘Western liberal’ morality is superior to a ‘traditional conservative’ standpoint. However, it is generally regarded as the best explanation of how a child’s pragmatic sense of right and wrong potentially progresses to more generalized ethical codes of adulthood.
Alternative theories of moral development
The cognitive approach of Piaget and Kohlberg is often accused of ignoring the emotional component in moral development. This is integral to some of the alternative approaches to moral development discussed below.
Freudian psychodynamic theory and moral development
Freud proposed that control of innate, amoral impulses from infancy until around 4 years of age is tempered by assessing ‘what can be got away with’. At around 5 years of age, the conscience emerges out of identification with the words and deeds of one’s same-sex parent and internalizing his or her values. The self is punished for the ‘should-nots’ it commits, engendering guilt, while fulfilling moral obligations generates feelings of self-satisfaction and pride. Conscience thus comes to replace parental authority as an internal moral watchdog. Freud contended that sexual and aggressive impulses, which cannot be expressed, are forced out of conscious awareness (see defence mechanisms, pp. 215–216, and Ch. 11).
Behaviourism (conditioning)
Eysenck suggested that people typically learn from childhood to connect wrongdoing with punishment through memory of past associations; thereafter even anticipated or pondered misdeeds may arouse negative emotions such as fear and guilt. Similarly, good deeds may be associated with rewards such as praise and the pleasant feelings of self-congratulation that follow. Thus moral behaviour is usually ‘reinforced’ and becomes predominant.
Social observational learning theory
In the 1960s, Bandura emphasized the significance of other individuals, known as ‘models’, that people observe from childhood onwards and whose behaviour they come to emulate. These include relatives such as parents or siblings, acquaintances, sporting champions, celebrities and even fictional characters in various entertainment media. Factors influencing the likelihood of such ‘modelling’ include perceived similarities between observer and model, e.g. gender, age, ethnicity, culture, considerations of status and personal qualities, and whether the model’s behaviour has beneficial consequences.
Development of interpersonal bonds
This process occurs with particular intensity during preschool childhood, the nature of the experience being of possibly lifelong significance. Formation of such bonds is often referred to as ‘attachment’ (see Ch. 9). Their severance, whether temporary or permanent, is known as ‘separation’.
Infants tend to receive adult attention from the outset due to their natural attractiveness and the curiosity they arouse, as well as any parenting instinct they may evoke. By 6 weeks of age infants will smile at human faces, then after 3 months seem able to distinguish familiar ones from those of strangers, becoming increasingly uncomfortable in the presence of the latter. They engage in active exchanges of expression, such as mutual gazing for continuous 20-second periods and reciprocal smiling, and seem able to detect differing moods in others through facial scrutiny, e.g. they appear perplexed if mother maintains a blank expression.
By 6 or 7 months of age, it has been held that children start to form a lasting emotional bond or attachment to one specific adult, usually the natural mother. Increasing attachment may develop until the child is nearly 3 years old (Bowlby 1988). This is apparent from the child attending to and seeking attention from this figure, and craving constant physical closeness to them. The toddler typically shows distress on separation and relief when reunited. Accordingly, Bowlby described attachment behaviour as the child’s ‘first love affair’.
In the 1950s, it was suggested that infants become attached to the person who feeds them, i.e. they are essentially motivated by the need to secure nourishment. As the child has to rely on its mother to satisfy primary drives (see p. 188) such as hunger and thirst, it develops a secondary drive for this servicing figure.
However, Harlow’s work with infant Rhesus monkeys who had been separated from their mothers and other monkeys at birth suggested otherwise. They preferred to cling to a cloth-covered contraption which rocked soothingly as a base rather than a wire ‘mother’ that contained their milk-feeding bottle, suggesting warmth and comforting physical contact to be the more powerful attraction.
In the next decade, it was argued that the attachment figure is the person who usually responds to the human infant’s behaviour in general and who is the main provider of stimulation. This might sometimes be the father, who perhaps returning from daytime occupational absence, and having little to do with feeding or comforting, becomes the child’s preferred playmate, the intense nature of his stimulating interactions, e.g. energetic games or bedtime story-reading, proving important in attaching his child to him. As the child grows older, it may develop multiple attachments, e.g. to grandparents, aunts and uncles, older siblings, neighbours and nursery carers, facilitating substitution for maternal absences with a minimum of emotional upset.
The significance of attachment
It could be that fear of strangers, some of whom might be ill-intentioned, and of isolation from the dependable adult that provides care has significant survival value to a vulnerable youngster. The latter also acts as a safe base from which to explore other things, places and people, so paving the way for future detachment and self-sufficiency.
Bowlby believed that continuous, individual loving care in early childhood was a prerequisite for developing interpersonal trust and fulfilling emotional relationships in adulthood. It is therefore crucial to a person’s future social competence, happiness and mental health, as important to the latter as nutrients are to physical health.
Reactions to separation from the attachment figure
In the 1950s, filmed evidence from research by James and Joyce Robertson on the distressed behaviour of hospitalized children startled many professionals involved in childcare (Box 8.27).
Separation anxiety
You may observe this occurring with your own children or during a nursery placement. Think of occasions when parents leave their children in the care of unrelated adults, for instance at nurseries or in hospital.
Subsequently, Bowlby described three behavioural stages exhibited by children in these circumstances:
The behavioural stages are reminiscent of those described in various models of loss and bereavement (see Ch. 12) and suggest that separation from the mother can be an emotionally traumatic experience for a preschool child. Bowlby used the term maternal deprivation to convey the effects of prolonged such separation, but this has been criticized for implying that only the mother is important in childhood attachment processes. Some specific situations where the implications of attachment are likely to be significant are discussed below.
Looked-after children, fostering and adoption
There has been concern about the effects of institutional care on orphans and whether children really need to form attachments to foster or adoptive parents early in life. In 1978, Tizard and Hodges observed that 4-year-olds cared for in institutions were over-friendly towards strangers and more ‘clingy’ towards carers. These children, however, seemed unselective and superficial in their attachments, displaying little emotion when staff members left (possibly a self-protection response following repeated separation or loss experiences) and quarrelsome with their peers (Hayes 2000). It was also reported that adopted children seemed to fare better scholastically and emotionally than those returned to their biological parents, although socioeconomic factors may partially account for this (Thomson & Meggitt 1997). Other studies suggest that adopted adolescents display significantly more adjustment and behavioural problems, unless adoption had occurred in infancy (Santrock 2004), and offer some support for Bowlby’s theory.
Working mothers
Dr Benjamin Spock expressed influential concerns in the 1950s that children might be damaged if deprived of essential continuous mothering. However, many children may benefit from the stimulation provided by substitute carers and other children in nurseries. Moreover, their mothers’ psychological as well as financial well-being may be significantly enhanced through working outside the home, through adult social contact and occupational stimulation. It may be observed that preschool children can form multiple attachments, including those with regular carers at nursery or child-minders, but they still show an obvious emotional preference for their returning parent.
Hospitalization
Separation due to hospitalization is stressful for both child and parents, whichever is the patient/client. Separation can occur in a wide variety of circumstances and hospitals now have a range of measures to minimize its psychological impact (Box 8.28, p. 214).
Reducing the effects of separation for parent and child in hospital
There is no disputing that separation due to hospitalization causes distress for children and their parents.
Student activities
[Resources: Action for Sick Children – www.actionforsickchildren.org Available July 2006; Chapter 11, e.g. Table 11.5]
Parental loss by death or divorce (see Ch. 12)
Bowlby’s theory would predict no difference in children’s emotional reaction to loss of a parent through death, parental break-up or abandonment, as all are essentially permanent separations from an attachment figure.
There have been suggestions that divorce increases the likelihood of antisocial behaviour, particularly in boys, as does separation from both parents, but only if this is preceded by prolonged and severe marital disharmony. This has led to the conclusion that amicable parting of parents is preferable for their children’s mental well-being than continuing marital strife (Hayes 2000). There are also well-established links between parental loss in childhood and depression (along with increased risk of divorce) in adulthood (McLeod 1991).
Variations in the attachment process
Ainsworth et al (1978) distinguished between:
Secure attachment has been linked to social assurance and emotional balance, and regarded as a kind of psychological ‘immune system’ for future mental resilience (Holmes 2001). Other factors such as later life experiences and family stressors are, however, likely to be significant, and insecure attachment does not invariably foreshadow future psychological problems.
The nature of the attachment relationship appears to stem partly from the parent’s approach. If it is consistently loving, responsive and sensitive, the secure pattern is likely to follow. If neglectful, critical or abusive, the insecure forms seem likelier. The child itself may also influence it, e.g. an unwell child tends to demand more parental interventions, and the young child’s personality may also be significant. Thomas and Chess (1977) described three types of infant temperament or natural predisposition:
Such early characteristics do not seem to be reliably reflected in a child’s adult personality. Parents may also vary in their preferences regarding their child’s temperament. A mother who lacks confidence might be reassured about her competence by an easy infant, while one domineered as a child herself may welcome the assertive behaviour of a difficult baby.
Culture and genetics may also be of significance. Chinese infants appear much more restrained, calm and easily soothed than Caucasian ones. This could reflect inherited characteristics or the value placed by the Chinese culture on self-control. Chinese–American parents are reported as less likely than those of other North American racial groups to encourage their infants’ smiling and vocalizing, or independent play (Bernstein et al 2003). Such factors are likely in turn to influence the nature of the attachment process.
Freud’s psychodynamic theory
Sigmund Freud (1856–1939) worked for most of his life in Vienna, first as a neurologist, then a psychiatrist, publishing numerous works to explain his treatment, known as psychoanalysis, and its underpinning psychodynamic theory. The latter viewed mental life as much influenced by continuous interplay between three active and largely unconscious structures, namely the:
The id comprises the inborn source of a person’s mental energy, generated by two antagonistic inherited instincts, Eros and Thanatos (p. 187). Eros represents the positive life-drive, whose energy, the libido, impels behaviour conducive to survival and reproduction. As meeting such needs is associated with self-gratification, the id has been described as operating via the ‘pleasure principle’. The opposing Thanatos initiates negative impulses such as aggressive and self-destructive behaviour. Infants are regarded as functioning via pure id.
The ego develops in response to experience of real world constraints, as the child finds their demands increasingly unmet by reflex activity or the intervention of others. Practical strategies have to be devised to satisfy id impulses in accordance with parental expectations and social rules. As it leads to compromise to gain an individual’s end, the ego operates on the ‘reality principle’, i.e. what actions a person is likely to get away with.
Growing exposure to and identification with the values of parents and significant others promotes their adoption or internalization as the system of ethical principles known as the superego, effectively one’s conscience (p. 212). This then compels the ego to obey the dictates of conscience and act in accordance with the new governing ‘morality principle’.
A person’s basic wants (id), practical options (ego) and moral considerations (superego) often conflict, causing a build-up of tension in the ‘pressure cooker’ of the unconscious (mind). Squeezed between the incessant demands of the id below and the inhibitions of the superego above (Fig. 8.6), the ego has to formulate an interminable series of behavioural compromises. Freud suggested that the outcome determines each person’s personality and mental health.

Safety valves
In order to protect the ego from being overwhelmed, Freud suggested that two principal methods of pressure (steam) release develop: dreaming and defence mechanisms.
Dreaming is a disguised method of expressing often-unacceptable desires, or wish-fulfilment. Intense fears can also be enacted during sleep, although the true meaning of the experience is concealed from the dreamer by the rich symbolism involved as well as loss of recall on awakening. Interpretation of dreams became a major tool of psychoanalysis.
Defence mechanisms are a series of unconscious tactics by which the ego can prevent unpleasant emotions from troubling the conscious mind. Each involves self-deception and distortion of reality, and can at best provide temporary respite rather than a true solution to the underlying problem (see Ch. 11 for more information about defence mechanisms in stress and coping). Some of the main defence mechanisms are:
Even if repressed out of conscious awareness, covert thoughts and impulses may occasionally surface in the form of slips of the tongue known as ‘Freudian slips’; memory lapses, e.g. of unwanted events or responsibilities; or physical mishaps, e.g. damaging disliked objects, all of which suggest to Freudians that there is no such thing as an innocent accident.
However, if the lid is kept too firmly on unconscious turmoil, the energy of the suppressed anxieties may be converted into emotional and physical ailments (previously known as psychosomatic). Box 8.29 (see p. 216) provides an opportunity to identify the defence mechanism operating in a series of scenarios.
Which defence mechanism?
Scenarios
Psychosexual personality development
Freud believed that personality developed through a series of consecutive stages, each distinguished by the part of the body affording most contemporary stimulation and resultant pleasure. Particularly controversial, especially at the turn of the 19th century, was his contention that the stage-related gratification was sexual in nature, even in infants. Either insufficient or excessive enjoyment within a stage could result in fixation there – remaining preoccupied with or continuing to indulge in the pursuits characterizing that period. This could be manifest in related traits and activities during adulthood. Such primitive vestiges could become particularly pronounced during stressful episodes, when the individual might dramatically revert, or regress, displaying strikingly immature behaviour. According to Freud, there are five stages: oral, anal, phallic, latent and genital.
Oral stage (0–24 months)
This reflects Piaget’s sensorimotor intelligence (see p. 208) and is subdivided into two phases:
Freud regarded weaning to be the main goal by the end of the oral stage, and the most common problems as resulting from either early cessation of or protracted breastfeeding.
The effects of fixation in the ‘passive oral’ personality may result in behaviours such as being dependent (like an infant), demanding (wailing for attention), greedy or gluttonous, breast-obsessed and displaying sucking behaviours, e.g. smoking, imbibing alcohol to excess, pen- or thumb-sucking, with regression to this if highly stressed.
In the ‘active oral’ personality the effects may include talkative, prone to sarcasm or abusive outbursts, as if the mouth is used as a weapon, as well as gum chewing, pencil nibbling or nail biting if anxious.
Anal stage (2–3 years)
The focus changes to the process and structures of elimination, particularly of faeces. This stage also comprises two substages:
Routine continence is the main goal by the end of the anal stage. Toilet training can become a frustrating and ambivalent process for all concerned, with difficulties resulting from both prolonged incontinence and rigid, authoritarian supervision (see Chs 20, 21).
The effects of fixation early on, an ‘expulsive anal’ personality, may be characterized by a person who is untidy, messy, wasteful, generous, unpunctual, prone to coarseness and vulgarity in speech and humour.
If fixation is later, a ‘retentive anal’ personality results, and the person may be fastidious, hygiene obsessed, methodical, perfectionist, obsessive, restrained, miserly and obstinate.
Phallic stage (4–5 years)
The child now becomes fascinated with genitalia, their own and those of other people, leading to curiosity about the mechanism of reproduction as well as genital fond-ling. Adult disapproval often follows, complicated by increasing attraction to the opposite sex parent and hostility to that of the same sex. Freud termed this gravitation the ‘Oedipus complex’ in boys and the ‘Electra complex’ in girls.
The main goal is that the ‘mummy’s boy’ and ‘daddy’s girl’ complexes resolve naturally through gradual acceptance of and identification with the same sex parent. Common problems are continued sexual inwardness and parental preoccupation.
The effects of fixation may include a lifelong worship of one’s opposite sex parent and choosing love partners by their resemblance to that figure; a competitive, ambitious and boastful nature, demonstrating an unconscious need to surpass the same sex parent. Narcissism, the preoccupation with one’s own attractiveness and flirtatiousness, may reflect the self-directed and abstract nature of sexual impulses inherited from this stage, and another vestige may be difficulties relating to authority figures.
Latent stage (6–11 years)
This is the temporary submersion of preceding sexual preoccupations into unconscious undercurrents. The child appears immersed in their hobbies and school activities. Playmates are typically of the same sex, and revulsion is commonly expressed at any exhibitions of affection, nudity or sexual passion that they may encounter, e.g. on television or between parents.
The focus switches to scholastic and sporting prowess (see stage 4 of Erikson’s model below).
The effects of fixation include adult immersion in work, study or pastimes, sexual coldness or indifference to the presence of the opposite sex.
Genital stage (12 years and above)
With the onset of puberty, sexual impulses reappear in a more conscious and urgent form, requiring satisfaction in intimate relationships and eventually through physical intercourse. This urge remains throughout adult life, and Freud envisaged its ultimate fulfilment in the form of enduring monogamous love. Equally conventional was Freud’s view of males, both in social and sexual roles, as naturally aggressive, adventurous and dominant compared with female passivity, maternalism and domesticity.
The main goal is physical love and reproduction; in this stage fixation is desirable. However, earlier fixations can interfere with this goal.
Criticisms and benefits of the psychodynamic approach
Criticisms of Freud’s approach included a lack of scientific basis and subjectivity. Another criticism was directed at its pessimism about human nature, as being at core irrational, hedonistic and destructive, and irresponsibility in focusing on childhood sexuality, a charge whose intensity surprised Freud. In addition, it may offend modern sensibilities as inherently sexist and viewing males as behaviourally and anatomically superior.
However, the benefits of Freud’s approach may include:
Erikson’s stage theory of psychosocial development
In the 1950s, Erik Erikson explored the relationship between psychological and social development. He produced a framework in which personal development occurs via a natural series of eight stages, each dominated by a major issue or crisis presented by the social environment (Table 8.3, see p. 217). If the child, adolescent or adult resolves the contemporary challenge positively, then a sound foundation is established for progression to later stages, and a healthy personality and functioning are more likely. However, a relatively maladaptive response will result in poor resolution of the issue, psychological problems and diminished ability to cope with later crises. Erikson suggested that it is possible to rectify inadequate confrontation of an issue retrospectively, even if another stage’s time parameters are the ideal point at which to resolve that crisis (Box 8.30). Conversely, previously gained ground can be lost once chronologically beyond a stage, e.g. to lose as well as regain trust in life during adulthood.
Table 8.3 Erikson’s stages of psychosocial development (after Gross 2001)
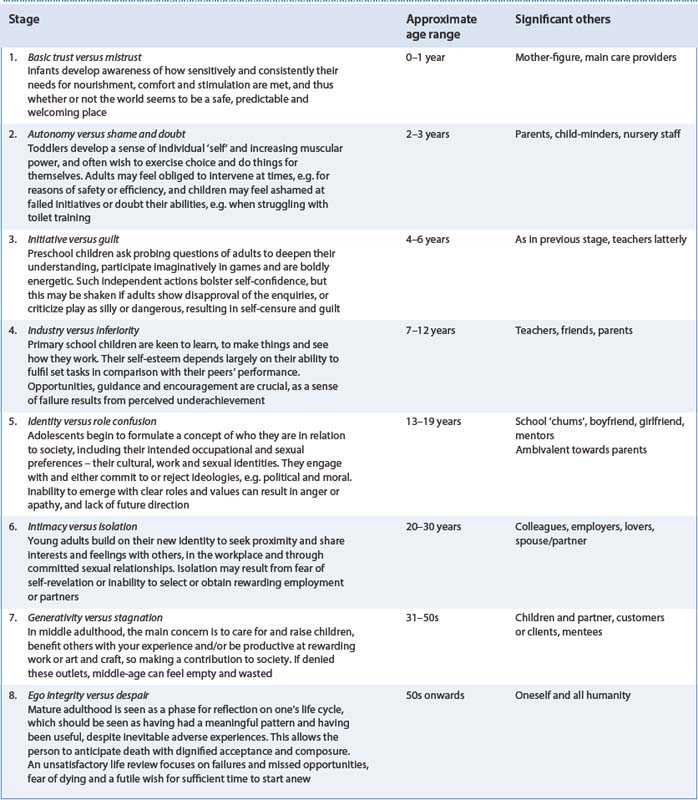
Erikson’s stages applied to nursing
Erikson suggested that people needed to make sense of and resolve typical challenges at whatever ‘stage’ of life they are.
| (i) self-actualization | (a) psychodynamic |
| (ii) self-destruction | (b) behaviourism |
| (iii) drive | (c) humanism |
Key words and phrases for literature searching
| Adaptation | Kohlberg |
| Ageing/aging | Motivation |
| Attachment | Normalization |
| Behaviourism | Norms |
| Cognitive | Piaget |
| Conditioning | Psychodynamic |
| Culture | Psychology |
| Development | Psychosexual |
| Developmental milestone | Psychosocial |
| Erikson | Role |
| Family | Self |
| Freud | Separation |
| Growth | Socialization |
| Humanist | Sociology |
| Intellectual | Values |
| Intelligence |
| BBC UK History | www.bbc.co.uk/history/timelines/britain/vic_indust_growth.shtml |
| Available July 2006 | |
| Scottish Recovery Network | www.scottishrecovery.net/content |
| Available July 2006 | |
| US National Library of Health MedlinePlus Medical Encyclopedia – provides information of developmental milestones at different ages | www.nlm.nih.gov/medlineplus/ency/encyclopedia_D-Di.htm |
| Available July 2006 |
Abercrombie N, Warde A. Contemporary British society, 3rd edn. Cambridge: Polity Press, 2005.
Ainsworth MDS, Blehar M, Waters E, Wall S. Patterns of attachment: a psychological study of the strange situation. Hillsdale, NJ: Erlbaum, 1978.
Alzheimer’s Society. 2006 Facts about dementia. Online: www.alzheimers.org.uk/Facts_about_dementia/Statistics/index.htm.
Atkinson RL, Atkinson RC, Smith EE, Bem DJ, Nolen-Hoeksema SN. Hilgard’s introduction to psychology, 13th edn, Fort Worth, TX: Harcourt; 2000:471.
Bee H, Boyd D. The developing child, 10th edn. Boston: Allyn & Bacon/Pearson Education, 2004.
Bernstein D, Penner LA, Clarke-Stewart A, Roy EJ. Psychology, 6th edn. Boston: Houghton Mifflin, 2003.
Bowlby J. A secure base: clinical applications of attachment theory. London: Routledge, 1988.
Denny E, Earle S. Sociology for nurses. Cambridge: Polity Press, 2005.
Denver Developmental Materials Inc. The Denver scale II. Denver: Denver Developmental Materials, 1990.
Eysenck MW. Psychology – a student’s handbook. Hove: Psychology Press, 2000.
Frankenburg WK, Dodds JB, Archer P, et al. The Denver II (developmental rating scale). Denver: Denver Developmental Materials, 1990.
Gates B, editor. Learning disabilities: toward inclusion, 4th edn, Edinburgh: Churchill Livingstone, 2002.
Giddens A. Sociology, 4th edn. Cambridge: Polity Press, 2001.
Goffman E. The presentation of self in everyday life. London: Penguin, 1971.
Gross RD. Psychology: the science of mind and behaviour, 5th edn. London: Hodder and Stoughton, 2001.
Hayes N. Foundations of psychology, 3rd edn. London: Thomson, 2000.
Haralambos M, Holborn M. Sociology: themes and perspectives. London: Harper Collins, 2005.
Hinchliff SM, Montague SE, Watson R. Physiology for nursing practice, 2nd edn. London: Baillière Tindall, 1996.
Holmes J. The search for the secure base. Hove: Brunner-Routlege, 2001.
Mader SS. Human biology, 6th edn. Boston: McGraw-Hill, 2000.
McLeod JD. Childhood parental loss and adult depression. Journal of Health and Social Behaviour. 1991;32(3):205-220.
Miell D. The self and the social world. Roth I, editor. Introduction to psychology, Vol. 1. Milton Keynes: Open University Press, 1990. Chapter 2
Napier University 1997. The individual, family and society: Module booklet 2. Edinburgh: Faculty of Health and Life Sciences, 2001.
Nursing and Midwifery Council. Code of professional conduct: standards for conduct, performance and ethics. London: NMC, 2004.
Santrock JW. Life-span development, 9th edn. New York: McGraw-Hill, 2004.
Thomas A, Chess S. Temperament and development. New York: Brunner and Mazel, 1977.
Thomson H, Meggitt C. Human growth and development for health and social care. London: Hodder and Stoughton, 1997.
Tizard B, Hodges J. The effect of early institutional rearing on the development of 8-year-old children. Journal of Child Psychology and Psychiatry. 1978;19:99-118.
Townsend P, Whitehead M. Inequalities in health: the Black report/the health divide. London: Penguin, 1990.
Watson D. Causes and manifestations of learning disabilities. In Gates B, editor: Learning disabilities: toward inclusion, 4th edn, Edinburgh: Churchill Livingstone, 2002. Chapter 2
Brooker C. Human structure and function, 2nd edn. London: Mosby, 1998.
Chamley C, Carson P, Randall D, Sandwell WM. Developmental anatomy and physiology of children. A practical approach. Edinburgh: Churchill Livingstone, 2005.
Denny E, Earle S. Sociology for nurses. Cambridge: Polity Press, 2005.
Durkin K. Developmental social psychology. In Hewstone M, Strobe W, editors: Introduction to social psychology: a European perspective, 3rd edn, Oxford: Blackwell, 2001.
Giddens A. Sociology. Cambridge: Polity Press, 1989.
Hockenberry MJ, Wilson D, Winkelstein ML, Kline N. Wong’s nursing care of infants and children, 7th edn. St Louis: Mosby, 2002. Chapter 7
Holmes J. John Bowlby and attachment theory. London: Routledge, 1993.
Light P, Oates J. The development of children’s understanding. Roth I, editor. Introduction to psychology, Vol. 1. Milton Keynes: Open University Press, 1990. Chapter 3
Montague SE, Watson R, Herbert R. Physiology for nursing practice, 3rd edn. Edinburgh: Baillière Tindall, 2005.
Thompson T, Mathias P, editors. Lyttle’s mental health and disorder, 3rd edn, Edinburgh: Baillière Tindall, 2000.